Overview
Neurological dysphagia, also called neurogenic dysphagia, is a swallowing problem that stems from a disruption in the nerves that control the muscles of the mouth, throat, and esophagus. Unlike a mechanical blockage (like a tumor), the issue is inside the wiring. Common culprits include stroke, Parkinsons disease, multiple sclerosis, amyotrophic lateral sclerosis (ALS), and traumatic brain injury. If your swallowing issues are linked to a broader neurologic diagnosis, resources on atypical Rett syndrome may be relevant when considering how complex neurodevelopmental conditions can affect feeding and swallowing.
Why does this matter? Swallowing may seem simple, but its a highstakes choreography. When the coordination falters, food or liquids can slip into the airway, leading to aspiration pneumonia, malnutrition, and a cascade of other health issues. Recognizing the symptoms early can make the difference between a quick adjustment and a serious medical emergency.
Core Symptoms
Food or pills feel stuck
Imagine a tiny pebble lodged at the back of your throat that wont budge, no matter how many sips of water you take. This lump in the throat sensation is one of the most common early clues of neurological dysphagia.
Coughing or choking on liquids
Liquids travel faster than solids, so a mistimed swallow often results in a sudden cough, gag, or a feeling that something went down the wrong pipe. This is a red flag for aspiration risk.
Prolonged meals
Do you find yourself spending 3045 minutes just finishing a plate? When the brain cant send the right signals, each bite becomes a laborintensive task, and you may need to rinse your mouth repeatedly.
Weight loss and fatigue
Quiet, unintentional weight loss is a sneaky symptom. If youre losing a few pounds without trying, it could be because youre not getting enough nutrition due to swallowing difficulties.
Voice changes after swallowing
A hoarse or nasal voice that appears right after a meal often signals that secretions are lingering in the airway.
Recurrent respiratory infections
Frequent colds, bronchitis, or pneumonia can be the bodys way of telling you that food or liquid is entering the lungs. A study published in links chronic dysphagia directly to these infections.
QuickCheck SelfAssessment
- Do you often feel a lump in your throat after meals?
- Do liquids make you cough or choke?
- Has your weight dropped without trying?
- Do you get sore throats or chest infections more often?
If you answered yes to two or more, its time to talk to a healthcare professional.
How It Differs
Oropharyngeal vs. Esophageal
| Aspect | Oropharyngeal Dysphagia | Esophageal Dysphagia |
|---|---|---|
| Location | Back of mouth & throat (pharynx) | Tube that connects throat to stomach (esophagus) |
| Typical Causes | Neurological disorders, stroke, Parkinsons | Acid reflux, strictures, cancer |
| Key Symptoms | Coughing, choking, feeling of food stuck in throat | Sensation of blockage lower down, heartburn, regurgitation |
| Diagnostic Tests | VFSS, FEES | Endoscopy, barium swallow |
Neurogenic vs. Mechanical
Neurogenic dysphagia means the nerves arent firing correctly, while mechanical dysphagia is a physical obstruction. The treatment pathways differ: neurogenic issues respond best to therapy and medication that target the underlying neurological disease, whereas mechanical problems might need dilation or surgery.
Is difficulty swallowing a sign of cancer?
Persistent dysphagiaespecially when accompanied by unexplained weight loss, blood in saliva, or paincan be an early warning sign of esophageal cancer. The good news is that most neurological dysphagia cases stem from noncancerous conditions. Still, never ignore a new or worsening swallowing problem; a prompt evaluation can rule out serious causes.
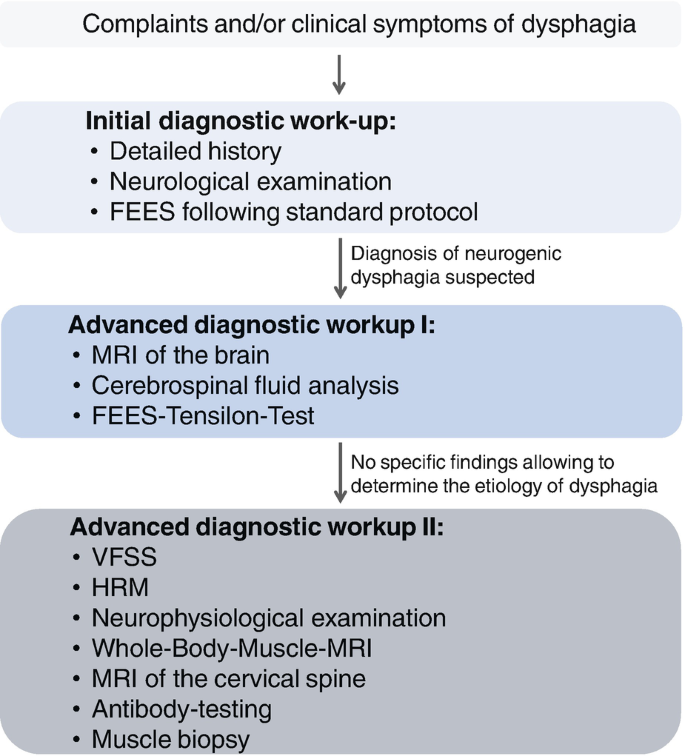
Diagnosing
Clinical swallow evaluation
The first step is usually a bedside swallow exam performed by a speechlanguage pathologist (SLP). Theyll watch you sip water, eat a slice of bread, and note any coughing or changes in voice.
Instrumental studies
Two goldstandard tests are the videofluoroscopic swallow study (VFSS) and the fiberoptic endoscopic evaluation of swallowing (FEES). VFSS captures Xray video of the swallow in real time, while FEES uses a tiny camera passed through the nose to directly view the throat.
Neurological workup
Depending on your history, doctors may order MRI or CT scans to locate lesions, or electromyography (EMG) to assess muscle activity. The aim is to pinpoint which part of the swallowing network is compromised.
When to see an SLP
If you notice any of the core symptoms, schedule an appointment with a certified SLP within a week. Early referral can dramatically improve outcomes and reduce the risk of aspiration pneumonia.
Managing Treatment
Swallowing therapy
Therapists teach exercises like the Mendelsohn maneuver (holding the larynx up) and effortful swallow techniques. These strengthen the muscles and improve timing. Think of it as a workout for the throatyes, it can be a little awkward, but the payoff is worth it.
Diet modifications
The International Dysphagia Diet Standardisation Initiative (IDDSI) provides clear levels: thin liquids, slightly thick, moderately thick, extremely thick, and pureed foods. Adjusting texture can make swallowing smoother while you work on the underlying deficit.
Medical and surgical options
In some cases, Botox injections can relax spastic muscles, and a cricopharyngeal myotomy can cut a tight muscle that blocks food passage. For severe cases where oral intake is unsafe, a percutaneous endoscopic gastrostomy (PEG) tube may be recommended.
Medications
There isnt a best medicine for dysphagia that cures the problem outright. Instead, medications target the root neurological diseaselevodopa for Parkinsons, diseasemodifying agents for multiple sclerosis, or antispasmodics for muscle tone. Proper medication management can indirectly improve swallowing. For patients navigating longterm neurological therapies, understanding coverage options such as Exondys 51 insurance may be important when planning treatment and support services.
Preventing complications
Good oral hygiene, upright sitting during meals, and meticulous pacing (small bites, alternating solids and liquids) lower the risk of aspiration. Some clinicians also advise using a chintuck posture for certain neurologic patterns.
Sample 7Day Meal Plan
- Day 1: Cream of oatmeal (moderately thick) + soft scrambled eggs
- Day 2: Pureed chicken stew with carrots, blended to smooth consistency
- Day 3: Mashed sweet potatoes, wellcooked fish, slightly thickened fruit puree
- Day 4: Smooth yogurt, pureed banana, and a protein shake (thin liquid)
- Day 5: Softcooked pasta with cheese sauce (moderately thick)
- Day 6: Pureed lentil soup, soft tofu, and applesauce
- Day 7: Cottage cheese, soft avocado mash, and honeysweetened tea (slightly thick)
All meals are served upright, with a 30second pause between bites.
LongTerm Outlook
Progressive vs. stable conditions
Some neurological diseases, like stroke, often plateau, allowing for significant improvement with therapy. Others, such as ALS, are progressive, and the focus shifts to maintaining safety and nutrition.
Redflag changes
Sudden worsening of choking, new weight loss, or repeated pneumonia episodes signal that your swallowing status has changed and warrants reevaluation.
Qualityoflife tools
The Swallowing Quality of Life (SWALQOL) questionnaire is a quick, validated survey that helps you and your care team track how dysphagia affects daily life. Keeping tabs on your scores can guide therapy adjustments.
Monitoring schedule
Most clinicians recommend a formal swallow reassessment every 612 months for stable conditions, and every 34 months for progressive diseases. Consistent monitoring catches subtle declines before they become emergencies.
Final Takeaway Summary
Neurological dysphagia may start with a simple lump feeling or a cough after a sip, but if left unchecked it can lead to serious complications like malnutrition and pneumonia. Recognizing the hallmark symptoms, getting a professional evaluation, and following tailored therapy can dramatically improve safety and quality of life. If any of the signs above sound familiar, dont waitreach out to your neurologist or a certified speechlanguage pathologist today. And remember, youre not alone; support groups, online forums, and knowledgeable clinicians are all ready to help you navigate this journey.
Whats your experience with swallowing difficulties? Have you tried any of the strategies mentioned? Share your story in the comments, and lets learn from each other.
FAQs
What are the most common neurological dysphagia symptoms?
Typical signs include choking or coughing on liquids, a sensation that food or pills are stuck in the throat, prolonged meal times, unintended weight loss, and voice changes after swallowing.
How can I tell if my dysphagia is neurogenic rather than mechanical?
Neurogenic dysphagia often presents with coughing, choking, or a “lump in the throat” feeling without pain or heartburn, whereas mechanical dysphagia is usually linked to blockage sensations lower in the esophagus and may involve pain or reflux.
When should I see a speech‑language pathologist for swallowing problems?
If you notice two or more of the core symptoms—especially choking on liquids, persistent food‑stuck feeling, or unexplained weight loss—schedule an appointment with a certified SLP within a week for an evaluation.
What lifestyle changes help reduce aspiration risk?
Adopt upright seating during meals, practice slow pacing with small bites, use appropriate food texture levels (per IDDSI), keep good oral hygiene, and consider posture techniques like the chin‑tuck for certain neurologic patterns.
Can medication improve neurological dysphagia?
There’s no drug that directly cures dysphagia, but treating the underlying neurological condition (e.g., levodopa for Parkinson’s) can improve muscle control and reduce swallowing difficulties.