If youve ever watched someone reach for a coffee mug and watch their hand miss the handle as if the world were a blurry puzzle, you might wonder whats really going on inside their head. The short answer: damage to both sides of the posterior parietaloccipital region is usually the trigger. In the next few minutes well walk through exactly which injuries, illnesses, and insults light the fuse for Balints syndrome, what the classic triad looks like, and what you can actually do about it.
What Is Balints?
What are the three classic signs?
Balints syndrome is famous for its triad: optic ataxia (trouble reaching for objects despite normal vision), ocular apraxia (difficulty moving the eyes voluntarily), and simultanagnosia (inability to perceive more than one object at a time). Imagine trying to read a page while you can only see one word at a time thats simultanagnosia in action.
How common is it?
Its a rare disorder roughly fewer than one case per 100,000 people. Because its so uncommon, many clinicians only see it a few times in their whole career. Yet when it does appear, it can be lifechanging, which is why understanding the cause matters.
Why should you care?
Beyond the medical curiosity, the syndrome can strip away independence. Simple tasks like buttoning a shirt or navigating a grocery aisle become hazardous. Knowing the cause helps you spot warning signs early and get the right help before frustration turns into fear.
Main Causes
Are strokes the biggest culprit?
Yes. Bilateral ischemic infarctions in the posterior parietaloccipital cortex especially watershed strokes that sit between major bloodsupply zones are the single most frequent trigger. Sudden drops in blood pressure or embolic clots can starve these vulnerable regions, sparking the full Balints picture almost overnight.
Can a head injury set it off?
Absolutely. Traumatic brain injury (TBI), whether from a car crash or a sports concussion, can produce diffuse axonal damage that hits both sides of the visualspatial network. A case report in PostTraumatic Balints Syndrome describes a young athlete who, after a severe concussion, suddenly couldnt accurately reach for a pencil.
What about other medical conditions?
Several less common diseases can masquerade as Balints:
- Posterior reversible encephalopathy syndrome (PRES) rapid bloodpressure spikes cause reversible swelling in the same posterior regions.
- Neurodegenerative disorders like Alzheimers disease or CreutzfeldtJakob disease, where the brain slowly erodes the parietal cortex.
- Infections, tumors, or demyelinating lesions that physically compress or infiltrate the area.
What about metabolic or toxic insults?
Severe hypoxia, carbonmonoxide poisoning, and even profound vitamin B12 deficiency have been linked to bilateral posterior damage, although theyre far rarer causes.
Associated Causes
How does Gerstmann syndrome relate?
Both syndromes involve the parietal lobe, but Gerstmann syndrome hits the angular gyrus (usually on one side) and produces a different set of symptoms: agraphia, acalculia, finger agnosia, and leftright disorientation. The overlap can confuse diagnosis, so clinicians keep a sidebyside symptom matrix handy.
Can neglect appear together?
Unilateral neglect (often after a righthemisphere stroke) focuses on one side of space, whereas Balints knocks out the ability to see the whole picture at once. Some patients show a hybrid picture, making the neuroexam a true detectives job.
Do genetics ever play a role?
Very rarely. A handful of familial cases have hinted at genetic predispositions, such as mutations in the NOTCH3 gene, but the evidence is still anecdotal.
How Its Diagnosed
What imaging do doctors order?
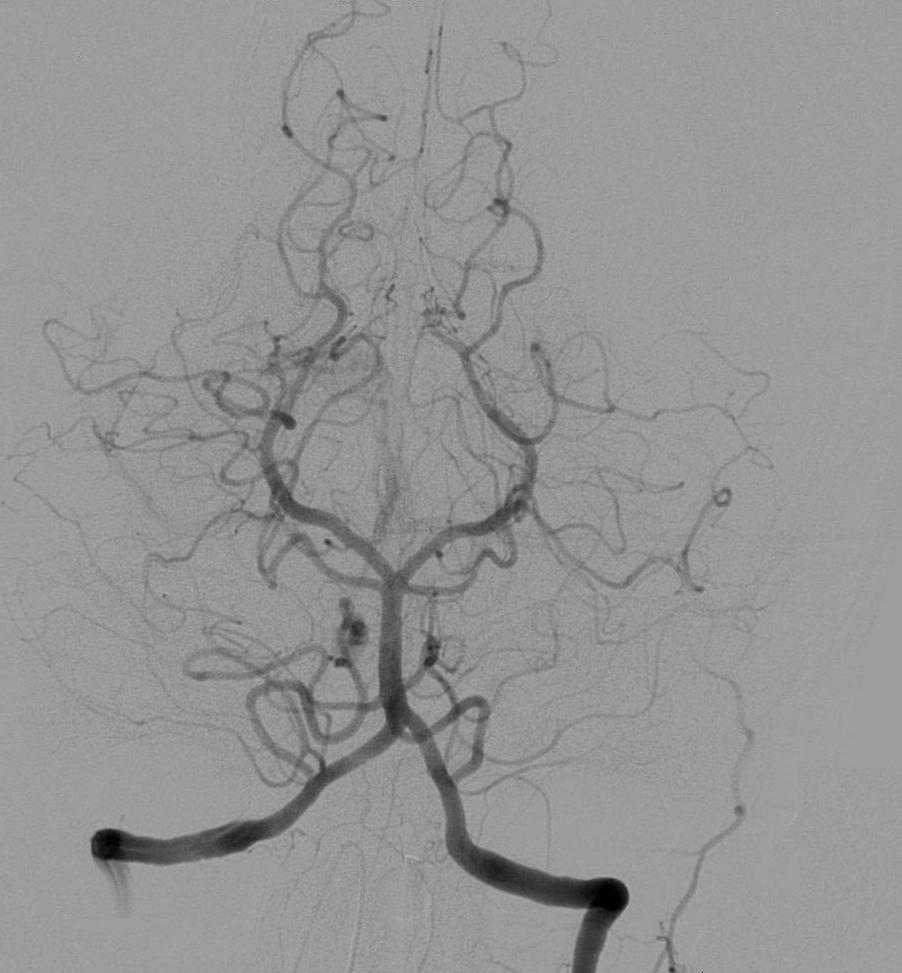
The gold standard is an MRI with T2FLAIR and diffusionweighted imaging (DWI). Youll typically see hyperintense lesions flanking both posterior parietal lobes. A quick look at a radiology report can confirm bilateral posterior cortical infarcts, the hallmark of Balints.
Which bedside tests reveal the triad?
For optic ataxia, clinicians ask patients to reach for objects placed in their visual field while their eyes stay fixed. Ocular apraxia shows up when a patient cant voluntarily shift gaze away from a fixed point even though the eyes move reflexively. Simultanagnosia is demonstrated with the Navon letters test large letters made of smaller letters; patients often see only the big letter.
How do neuropsychologists help?
Standard batteries include spatial orientation tasks and complex figure copying. The results add depth to the diagnosis and guide rehabilitation planning.
When are labs needed?
If the imaging doesnt explain the damage, doctors may order a CBC, metabolic panel, and sometimes a lumbar puncture to rule out prion disease or infectious etiologies.
Treatment Options
What can be done for acute strokes?
Time is brain. Intravenous thrombolysis (tPA) or mechanical thrombectomy, if youre within the therapeutic window, can restore blood flow and limit permanent loss. Even when the damage is already done, aggressive bloodpressure control and secondaryprevention drugs (antiplatelets, statins) lower the risk of a second hit.
Is there a specific Balints therapy?
Not a magic pill, but targeted rehabilitation makes a real difference. Visionspatial occupational therapy teaches patients to break tasks into smaller, manageable steps. Eyemovement training, often using computerbased saccade exercises, helps reduce ocular apraxia over weeks.
What medications might help?
If the underlying cause is Alzheimers, cholinesterase inhibitors can modestly improve cognition, which indirectly eases visualspatial deficits. For poststroke seizures, antiepileptics are prescribed. No drug directly cures Balints, but managing the root condition is crucial.
When is surgery an option?
Only in rare cases where a tumor or vascular malformation is compressing the posterior cortex. Even then, surgeons weigh the risks of further damaging the delicate visualspatial network.
How can families keep patients safe?
Simple home modificationsremoving lowlying obstacles, adding extra lighting, and using contrasting colors for objectscan prevent falls. Driving assessments are essential; many patients need to relinquish their license until visualspatial skills improve.
Quick Reference Table
| Cause | Typical Imaging | Onset | Associated Condition |
|---|---|---|---|
| Bilateral watershed infarct | DWI hyperintensity in posterior parietal lobes | Acute (minuteshours) | Hypertensive crisis |
| Traumatic brain injury | Contusions/hemorrhage in occipitalparietal region | Acutesubacute | Postconcussive syndrome |
| PRES | Reversible vasogenic edema | Acute | Severe hypertension, eclampsia |
| Alzheimers disease | Cortical atrophy with posterior predominance | Chronic | Dementia |
| CJD | Ribbonlike cortical hyperintensity | Rapidly progressive | Prion disease |
Bottom Line
In short, Balints syndrome pops up when both sides of the brains visualspatial hub get hurt most often by a sudden stroke or a nasty blow to the head. Other culprits like PRES, neurodegeneration, or rare metabolic insults can join the party, but they all share the same final pathway: bilateral posterior damage. Early MRI and a focused bedside exam are the fastest routes to a solid diagnosis. Treat the root cause (revascularize a stroke, control blood pressure, manage an underlying disease) and pair that with dedicated visionspatial rehab to give patients the best shot at regaining independence.
Whats your story? Have you or someone you love faced the baffling world of Balints syndrome? Share your thoughts below or reach out to a neuroophthalmology specialist the sooner you get the right help, the sooner you can start seeing the whole picture again.