Is your child showing some Rettsyndrome traits but not the full picture? Atypical Rett syndrome is the name doctors use when only part of the classic criteria are met, and understanding its nuances can help families get the right diagnosis, care, and hope.
Overview
What Is Atypical Rett Syndrome?
Atypical Rett syndrome (often shortened to atypical RTT) is a neurodevelopmental disorder that shares many hallmark features with classic Rett syndromesuch as loss of purposeful hand use and speech regressionbut it doesnt tick every box on the official diagnostic checklist. Think of it as the cousin of classic RTT, walking a slightly different path while still needing the same amount of love, support, and medical attention.
Why Does the Term Atypical Matter?
The word atypical isnt meant to diminish the seriousness of the condition. Instead, it signals to clinicians that the childs symptoms may appear sooner, later, or in a slightly different combination than the classic form. This matters because treatment plans, therapy goals, and even the outlook can shift based on whether a child fits the classic or atypical pattern.
Key Statistics
Current estimates suggest that atypical RTT accounts for roughly 2030% of all Rettsyndrome diagnoses, with girls being the most commonly affected gender due to the Xlinked nature of the underlying genetic mutations. Sources such as the provide uptodate prevalence figures.
Differences
Classic vs. Atypical Rett Syndrome
| Feature | Classic RTT | Atypical RTT |
|---|---|---|
| Age of onset | 618 months | Can be earlier or later, sometimes after 2years |
| Hand stereotypies | Present in >90% | Often present but may be milder |
| Speech loss | Almost universal | May retain some speech (Preserved Speech variant) |
| Breathing irregularities | Frequent hyperventilation/apneas | Less common, variable |
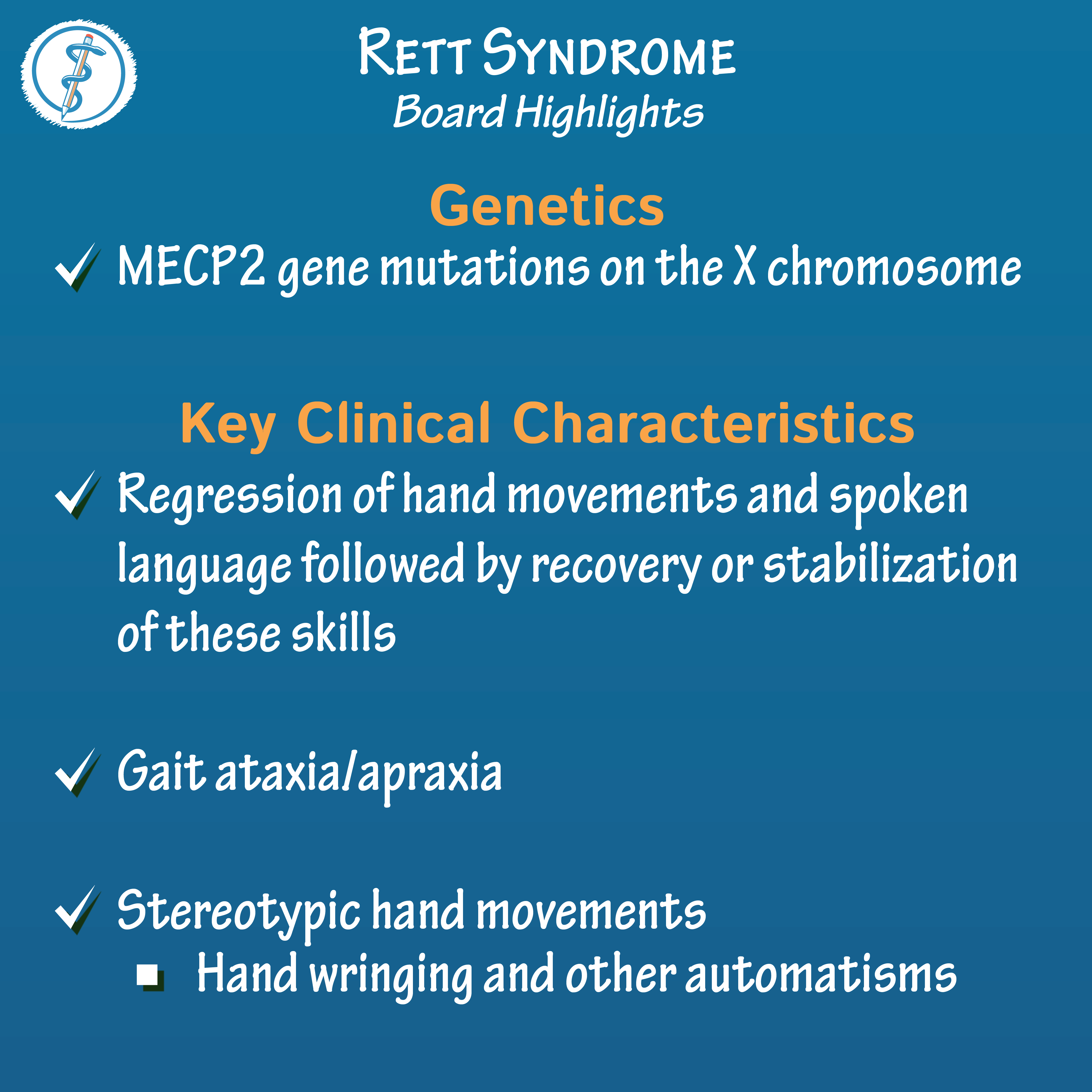
| Genetic mutations | MECP2 >99% | MECP2, CDKL5, FOXG1 (mixed) |
The Five Recognised Atypical Variants
Researchers have identified several subtypes that help clinicians finetune their approach:
- Forme Fruste Rett Syndrome the mild presentation, sometimes barely noticeable.
- Zappella Variant preserved speech, relatively better motor function.
- Hanefeld Variant early onset seizures dominate the picture.
- EarlyOnset Seizure Variant seizures appear within the first year.
- Preserved Speech Variant children keep functional language longer.
Common Misconceptions
Its easy to assume atypical = milder, but thats not always true. Some atypical forms, especially those involving early seizures (the Hanefeld variant), can be just as challenging as classic RTT. The key is to look at the whole childnot just the label.
Signs
Core Symptoms That Overlap
Both classic and atypical Rett share a core trio:
- Developmental regression after a period of apparently normal growth.
- Loss of purposeful hand use, often replaced by repetitive handwringing or clapping.
- Decline in spoken language.
Features That May Be Absent or Milder
In atypical cases you might see:
- Less severe breathing problems.
- More preserved gait or ability to walk.
- Partial retention of expressive language (especially in the Preserved Speech variant).
When to Suspect Atypical RTT
Heres a quick redflag checklist you can run through with your pediatrician:
- Developmental milestones are hit, then suddenly stall or reverse.
- Handclapping or wringing appears without a clear trigger.
- Speech seems to fade, but some words or phrases linger.
- Seizures start early (often before age2) and are hard to control.
- Family history of MECP2, CDKL5, or FOXG1 mutations.
RealWorld Example
Emily, a 3yearold, was thriving until she stopped using her favorite crayons and began repeatedly clapping her hands. Her parents thought it was a phase, but a neurologist recognized the pattern and referred them for genetic testing. Within weeks they learned Emily had the Preserved Speech variant of atypical Rettinformation that opened doors to targeted speech therapy and a support network.
Diagnosis
Diagnostic Criteria (2023 Update)
The most recent guidelines, published by the , require at least two of the four main criteria (developmental regression, loss of hand skills, loss of spoken language, gait abnormalities) plus supportive findings such as a pathogenic mutation in MECP2, CDKL5, or FOXG1.
Genetic Testing Workflow
When a clinician suspects atypical RTT, the typical pathway looks like this:
- Step1: Clinical evaluation detailed developmental history and physical exam.
- Step2: Targeted gene panel testing for MECP2, CDKL5, FOXG1.
- Step3: Wholeexome sequencing if the panel is negative but suspicion remains high.
Results can be pathogenic, likely pathogenic, or variant of uncertain significance. A genetic counselor helps families interpret what each outcome means for treatment and family planning.
Rett Syndrome Diagnosis Test: What the Specialist Looks For
Besides genetics, doctors run a battery of assessments:
- Neurological exam focusing on hand stereotypies.
- Speechlanguage evaluation to gauge retained abilities.
- EEG to detect seizure patterns, especially in the earlyonset variant.
- Respiratory monitoring for subtle breathing irregularities.
Sample Lab Report Walkthrough
Imagine a report that reads: MECP2 c.473C>T (p.Arg158*) pathogenic. This tells you that a singleletter change in the MECP2 gene creates a stop codon, truncating the protein and leading to Retttype symptoms. The report will also note whether the mutation was inherited or de novo.
Prognosis
Atypical Rett Syndrome Life Expectancy
While life expectancy varies, most studies indicate that individuals with atypical RTT live into their 40s or beyond, especially when seizures and respiratory issues are wellmanaged. A 2022 cohort study published in Neurology found a median lifespan of 45years for atypical cases, compared with 38years for classic RTTa modest but hopeful difference.
Factors That Influence Outcomes
Several variables can tip the scales toward a better quality of life:
- Early detection and intervention (speech, occupational, physiotherapy).
- Effective seizure controloften the biggest mortality driver.
- Access to multidisciplinary care (neurology, genetics, nutrition).
- Family and community support networks.
Comparing Stage4 Classic RTT vs. Atypical Stage4
| Aspect | Classic RTT Stage4 | Atypical RTT Stage4 |
|---|---|---|
| Mobility | Mostly wheelchairbound | Often retains limited walking ability |
| Communication | Nonverbal, limited eyegaze | May retain a few words or gestures |
| Seizure Frequency | High, often refractory | Variable; some variants have fewer seizures |
| Breathing Irregularities | Prominent (hyperventilation/apnea) | Less severe, intermittent |
Stages
The 4 Stages of Rett Syndrome Can They Apply to Atypical?
The classic model divides Rett into four stages: early onset, rapid regression, plateau, and late motor deterioration. In atypical RTT, the timeline can be stretched or compressed, and not every child will hit all four stages in the same order. Nevertheless, the framework remains useful for tracking progress and planning interventions.
LateChildhood Rett Syndrome: What Families See
By the time children reach the latechildhood window (roughly ages812), many have settled into a plateau phase. Hand stereotypies may lessen, and some regain limited purposeful hand use. However, challenges such as scoliosis, mobility issues, and learning difficulties often become more pronounced.
Milestones to Monitor at Each Stage
- Stage1 (06months): Watch for subtle delays in reaching milestones.
- Stage2 (624months): Look for regression in language or hand skills.
- Stage3 (210years): Stabilization; focus on therapy goals.
- Stage4 (adolescence onward): Manage motor decline and secondary health issues.
Management
Medical Management
Medication is usually aimed at controlling seizures and managing breathing irregularities. Common antiepileptic drugs include valproic acid, levetiracetam, and, in refractory cases, the ketogenic diet. Respiratory support can range from nighttime CPAP to, rarely, tracheostomy in severe apnea.
Therapies That Make a Difference
Multidisciplinary therapy is the cornerstone of care:
- Speech therapy even limited speech benefits from augmentative communication devices.
- Occupational therapy targets hand function, splinting, and finemotor skill development.
- Physical therapy focuses on gait, balance, and preventing contractures.
- Behavioral support helps families cope with stress, anxiety, and the daytoday challenges of caregiving.
Emotional Support for Families
Its okay to feel overwhelmed. Parenting a child with atypical RTT can feel like walking a tightropebalancing medical appointments, therapy sessions, and everyday life. Support groups, both inperson and online, provide a safe space to share triumphs and setbacks. The runs monthly webinars that many families find reassuring.
Useful Resources & Support Groups
- National Organization for Rare Disorders (NORD) patient guides.
- Rett Syndrome Foundation clinical trial listings.
- Local Rare Disease Coalitions advocacy and financial assistance.
Further Reading
Citing TopTier Sources
When you dive deeper, look for peerreviewed articles from journals like Brain and Neurology, as well as guidelines from reputable organizations (e.g., the ). These sources keep the information trustworthy and uptodate.
Recommended Scientific Papers
Some recent studies worth a read:
- MEMECP2 Mutations and Phenotypic Spectrum in Atypical Rett Journal of Medical Genetics (2023).
- LongTerm Outcomes in Atypical Rett Syndrome Neurology (2022).
- Seizure Management Strategies in CDKL5Related Disorders Epilepsia (2021).
How to Stay Updated
Medical knowledge evolves quickly. Consider signing up for email alerts from the Rett Syndrome Foundation, following clinicaltrial registries on ClinicalTrials.gov, and subscribing to raredisease newsletters. Staying informed gives you a stronger voice when discussing options with your childs care team.
Conclusion
Understanding atypical Rett syndrome helps families move from uncertainty to action. By knowing the signs, the diagnostic pathway, and the realistic outlook, you can partner with specialists, access the right therapies, and connect with a supportive community. If you suspect atypical RTT or want more personalized guidance, reach out to a genetics clinic or a certified Rettsyndrome center today. Stay informed, stay hopeful, and remember youre not alone on this journey.
FAQs
What differentiates atypical Rett syndrome from classic Rett syndrome?
Atypical Rett syndrome meets only some of the classic diagnostic criteria, often showing milder hand stereotypies, retained speech, or a different age of onset, whereas classic RTT displays a full set of hallmark features.
Which genetic mutations are most commonly associated with atypical Rett syndrome?
The condition is most frequently linked to mutations in MECP2, but CDKL5 and FOXG1 mutations are also seen, especially in specific atypical variants.
How is atypical Rett syndrome diagnosed?
Diagnosis involves clinical evaluation for core symptoms, supportive testing (EEG, respiratory monitoring), and genetic testing—starting with a targeted panel for MECP2, CDKL5, and FOXG1, followed by whole‑exome sequencing if needed.
What are the main treatment approaches for atypical Rett syndrome?
Treatment is multidisciplinary: anti‑epileptic drugs for seizure control, speech and occupational therapy to maximize communication and hand function, physical therapy for mobility, and respiratory support when required.
What is the long‑term outlook for children with atypical Rett syndrome?
With early intervention and effective seizure management, many individuals live into their 40s or beyond; quality of life improves with ongoing therapy, multidisciplinary care, and strong family support.