Thinking about a heartvalve replacement can feel like staring at a huge, confusing road map. The good news? There are just a few main routes, and each one has clear signs that tell you when its the right fit. Below youll find a friendly walkthrough of the most common valve replacement options, the pros and cons, and how doctors decide which path makes the most sense for you.
Quick Overview
What is a heartvalve replacement?
A heartvalve replacement is a surgical or catheterbased procedure that removes a diseased valve and puts a new one in its place. The goal is simple: restore smooth blood flow and ease symptoms like shortness of breath or fatigue.
Why replace instead of repair?
When a valve is severely narrowed (stenosis) or leaky (regurgitation), repairing it often isnt enough to bring back normal function. In those cases, swapping the valve for a fresh prosthetic gives the heart a clean slate.
Key stats (20242025)
According to the Mayo Clinic, more than 300,000 valve replacements are performed in the United States each year, and that number is climbing as imaging gets better and patients live longer.
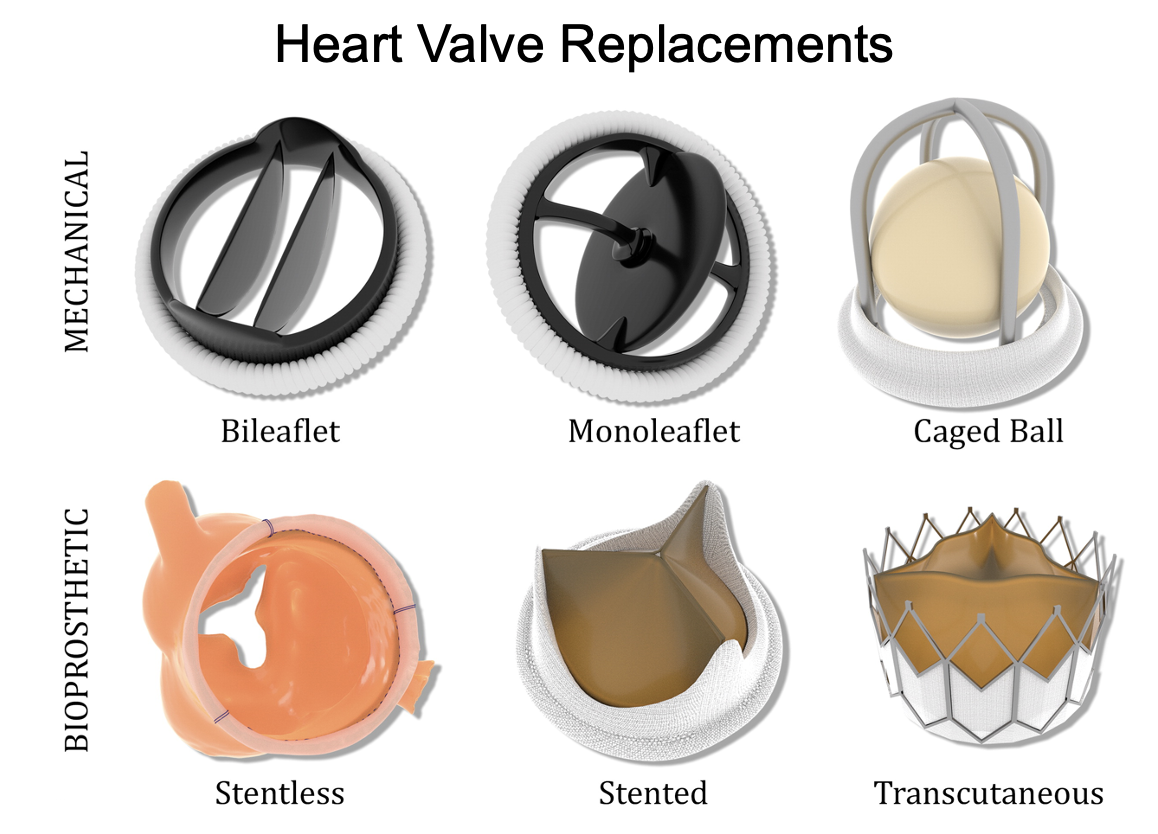
Valve Types
Mechanical valves (durable)
Mechanical prostheses are made from carboncoated titanium or other tough metals. Theyre built to lastoften 2030 years or moreso theyre a popular choice for younger patients who want to avoid a second operation.
Pros
- Longest durability on the market.
- Lower chance of needing a repeat surgery.
Cons
- Require lifelong blood thinners (usually warfarin) to prevent clots.
- Higher risk of bleeding complications.
Biological (tissue) valves
These come from animal tissuemost often pig (porcine) or cow (bovine pericardial) sourcesor from donated human hearts (homografts). Theyre called tissue or biological valves because theyre harvested and treated to become a living, flexible substitute.
Pros
- No permanent anticoagulation for most patients.
- Quicker recovery and fewer lifestyle restrictions.
Cons
- Usually last 1015 years, after which they may need replacement.
- Potential for structural valve deterioration over time.
Transcatheter valve replacement (TAVR/PCI)
Ever wondered can a heart valve be replaced without openheart surgery? The answer is yesthrough a minimally invasive catheterbased method called transcatheter aortic valve replacement (TAVR). A tiny valve is crimped onto a balloonlike catheter and guided through a blood vessel (often the femoral artery) to the heart, where it expands and takes over the job of the diseased valve.
This approach is especially popular for older adults or patients deemed highrisk for traditional surgery. The Cleveland Clinic reports that TAVR now accounts for roughly onethird of all aortic valve replacements in the U.S.
How Surgery Works
Openheart (median sternotomy)
The classic route involves a vertical incision down the breastbone, followed by a heartlung machine that takes over circulation while the surgeon removes the old valve and sews the new one in place. The whole process usually takes 35 hours.
Minimally invasive (partial sternotomy, minithoracotomy)
Instead of a full split, surgeons can make a smaller Jshaped cut or a sideentry between the ribs. The result? Less pain, a shorter ICU stay, and a faster return to everyday activities.
Transcatheter (femoral or transapical)
During a TAVR procedure, the patient is usually sedated rather than fully anesthetized. A catheter slides up the groin or chest, and the new valve is carefully positioned using realtime imaging. Once the valve is deployed, it immediately begins workingno need to stop the heart.
Risks & Success
Overall success rate
Modern valve replacement surgery boasts a 30day survival rate of 9598%, according to the American College of Cardiology. Longterm durability depends on the type of valve and the patients age.
Complication profile by valve type
| Valve Type | Key Risks |
|---|---|
| Mechanical | Bleeding (from anticoagulation), thromboembolism, rare valve thrombosis. |
| Biological (tissue) | Structural valve deterioration, endocarditis, occasional need for reoperation. |
| Transcatheter (TAVR) | Vascular injury, paravalvular leak, need for pacemaker implantation. |
Agerelated considerations
When you ask what is the average age for heart valve replacement? the answer varies:
- Mechanical valves: Usually recommended for patients<60years old.
- Biological valves: Most common in the 6075year range.
- TAVR: Dominates for patients70years or anyone at high surgical risk.
Theres no hard age limit for replacement; the decision hinges on overall health, lifestyle, and personal preferences.
Choosing Right Option
Decision factors at a glance
| Factor | Mechanical | Biological (Tissue) | Transcatheter (TAVR) |
|---|---|---|---|
| Durability | 2030years | 1015years | 1012years (varies) |
| Anticoagulation | Lifelong warfarin | Usually none | Usually none |
| Typical Age | <60yr | 6075yr | 70yr or highrisk |
| Lifestyle Impact | Restrictions on contact sports | Fewer limits | Fast recovery, minimal scar |
| Reoperation Risk | Low | Moderate | Moderatehigh |
Patientcentered questionnaire
Take a minute and answer these quick yes/no questions. Your answers will point you toward the valve type that feels most comfortable:
- Are you willing to take a daily blood thinner for the rest of your life? (Yesmechanical)
- Do you prefer a shorter recovery and no lifelong medication? (Yesbiological or TAVR)
- Is staying active in highimpact sports important to you? (Yesmechanical)
- Do you have other health conditions that make major surgery risky? (Yesconsider TAVR)
- Would you like to avoid a possible second surgery in the next 1015 years? (Yesmechanical)
HeartTeam approach
Modern cardiac care isnt a solo act. A heart teamincluding a cardiothoracic surgeon, interventional cardiologist, cardiac imaging specialist, and often a nurse practitionerwill sit down with you, review your imaging, labs, and lifestyle, then recommend the best valve replacement option. This collaborative model is championed by the Mayo Clinic and has been shown to improve outcomes.
PostOp Care & Lifestyle
Medication management
If you receive a mechanical valve, youll start warfarin and will need regular INR checks to keep your bloods clotting ability in the right range. Tissuevalve patients might only need a short course of antiplatelet therapy, and TAVR recipients often take dual antiplatelet drugs for a few months.
Activity guidelines
Most patients can walk around the hospital the day after a minimally invasive or TAVR procedure. Fullstrength exercise usually resumes within 46 weeks, though highimpact sports are still offlimits for mechanicalvalve recipients.
Imaging surveillance
Echo checks are the gold standard. Your doctor will typically schedule a transthoracic echo at 6months, again at 1year, and then annually to monitor valve function and spot any early wear.
When to call the doctor
Watch for sudden shortness of breath, chest pain, fever (possible endocarditis), or unexplained bruising/bleeding if youre on anticoagulants. Prompt evaluation can prevent minor issues from becoming major.
Bottom Line & Next Steps
Choosing a valve replacement option is a balancing act between durability, medication burden, age, and lifestyle. Mechanical valves give you the longest lifespan but lock you into blood thinners. Biological (tissue) valves spare you the daily pills but may need a redo in a decade or so. Transcatheter approaches let many older or higherrisk patients avoid a full chest opening, though theyre not yet the default for younger folks.
The best path forward is a conversation with a multidisciplinary heart team that weighs your personal health goals against the evidence. If youre ready to explore your options, download our printable decisionaid checklist (link at the end of this page) or schedule a consultation with a cardiac specialist today. Your heart deserves a plan thats as unique as you are.
FAQs
What are the main types of valve replacement options?
The primary options include mechanical valves, biological (tissue) valves, and transcatheter valve replacement (TAVR).
How long do mechanical valves typically last?
Mechanical valves can last 20‑30 years or more, often outliving the patient.
Do I need lifelong blood thinners with a tissue valve?
Most tissue‑valve recipients avoid permanent anticoagulation; they may only need short‑term antiplatelet therapy.
Is TAVR suitable for younger patients?
Currently, TAVR is mainly recommended for patients 70 years or older or those at high surgical risk, though research is expanding its use.
What factors does the heart‑team consider when choosing a valve?
They evaluate age, comorbidities, lifestyle, anticoagulation tolerance, valve durability, and anatomical suitability.