Hey there! If youve landed on this page, chances are you (or someone you love) are looking for clear, trustworthy info about familial dysautonomia straight from the goldstandard GeneReviews source. Lets skip the jargonheavy preamble and dive right into what matters most: what the condition is, how it shows up, the genetics behind it, testing options, treatment, and living with it as an adult. Think of this as a chat over coffee, with a sprinkle of science to keep us precise.
What Is Familial Dysautonomia
Definition & Core Characteristics
Familial dysautonomia (FD), also known as Riley-Day syndrome, is a rare, inherited disorder of the autonomic nervous system. In plain English, the nerves that automatically control things like heart rate, blood pressure, digestion, and temperature regulation dont work the way they should. This leads to a distinctive set of symptoms that can appear as early as infancy.
Epidemiology & Who Gets It
FD is strikingly more common among people of Ashkenazi Jewish descent. The carrier frequency hovers around 1 in 27 in that population, while the overall prevalence is about 1 in 30,000 worldwide. Thats why youll often see the phrase familial dysautonomia carrier frequency pop up in genetic counseling sessions. For those outside the Ashkenazi community, the condition is exceptionally rare, but it can still occur due to other genetic variations.
| Population | Prevalence | Carrier Frequency |
|---|---|---|
| Ashkenazi Jewish | 1 in 30,000 | 1 in 27 |
| General Global | ~1 in 300,000 | Much lower |
Inheritance Pattern
FD follows an autosomal recessive inheritance. In simple terms, both parents must pass on a faulty copy of the ELP1 (formerly IKBKAP) gene for a child to develop the disorder. If only one copy is inherited, the person becomes a carrierhealthy but capable of passing the mutation to future generations.
Key Symptoms Overview
EarlyLife Signs
Babies with FD often struggle with feeding because the nerves that trigger the swallow reflex are offkilter. You might notice frequent vomiting, a lack of tears when they cry (yes, they can look dry even if theyre upset), and poor growth. These pivotal familial dysautonomia symptoms usually raise red flags within the first few months.
Childhood & Adolescent Features
As children grow, the autonomic imbalance continues to manifest. Common clues include:
- Gait instability and frequent falls
- Scoliosis (curved spine) due to muscle tone issues
- Bloodpressure crisessudden spikes or drops that can cause dizziness or fainting
- Pain insensitivity (they might not feel injuries right away)
AdultOnset Concerns
Adults with FD arent cured as they age, but the disease shapeshifts. Respiratory challenges, chronic pain, and dysautonomic crises tend to become the main concerns. A small but hopeful trend is that better multidisciplinary care is nudging life expectancy upward, something well explore shortly.
Symptom Checklist
- Feeding difficulties
- Absence of tears
- Unsteady gait
- Bloodpressure swings
- Pain insensitivity
- Respiratory issues (adults)
Genetics Made Simple
The ELP1 (IKBKAP) Gene
The star player in FD is the ELP1 gene, located on chromosome 9. A specific mutation, c.2204+6T>C, is responsible for roughly 99% of cases in the Ashkenazi Jewish community. This mutation hampers the production of a protein essential for the development and survival of autonomic neurons.
Types of Genetic Tests
When you or a loved one seeks answers, there are a few testing routes:
- Diagnostic sequencingusually done after symptoms appear; it directly looks for the ELP1 mutation.
- Carrier screeningrecommended for couples of Ashkenazi descent or anyone with a family history; its a quick blood or saliva test.
- Prenatal testingif youre pregnant, you can opt for chorionic villus sampling (CVS) or amniocentesis to check the babys DNA.
Interpreting Results
A positive diagnostic result means the person has two diseasecausing copiesFD is confirmed. A carrier result indicates one faulty copy; the individual is healthy but can pass the mutation on. A negative result means no detectable ELP1 mutation, though rare atypical variants could escape standard panels.
Sample Lab Report WalkThrough
Imagine opening a PDF that says ELP1 c.2204+6T>C Homozygous pathogenic. The homozygous part tells us both gene copies carry the mutation, confirming FD. If it reads heterozygous, thats a carrier status, and youd discuss family planning options with a genetic counselor.
Carrier Testing Guide
Who Should Consider Testing?
If youre of Ashkenazi Jewish heritage, have a family member with FD, or are part of a couple where one partner is a known carrier, its wise to explore carrier testing. Even if youre not from that background, a doctor might still recommend testing if you have unexplained autonomic symptoms in your child.
Carrier Frequency Statistics
According to the , about 1 in 27 Ashkenazi Jews carries the pathogenic ELP1 variant. In contrast, the carrier frequency in the general population is roughly 1 in 2,500. These numbers help put the risk into perspective when making reproductive choices.
Comparison Table: FD vs. General Dysautonomia Carrier Rates
| Condition | Carrier Rate (Ashkenazi) | Carrier Rate (General) |
|---|---|---|
| Familial Dysautonomia | 1 in 27 | 1 in 2,500 |
| General Dysautonomia | Varies (mostly nongenetic) | Not applicable |
Life Expectancy Insights
Median Survival Data
Historically, FD was considered a childhoodonly disease, with many patients not reaching adulthood. However, recent cohort studies (20232024) show a median survival into the mid40s, and a growing number of individuals are thriving into their 50s and beyond. Advances in respiratory support, nutritional management, and early genetic diagnosis have all contributed to this improvement.
Factors That Improve Outcomes
Think of life expectancy like a garden: the right care makes everything flourish. Key factors include:
- Early multidisciplinary careneurologists, gastroenterologists, pulmonologists, and physiotherapists working together.
- Proactive respiratory managementusing sleepstudies, noninvasive ventilation, and airway clearance techniques.
- Optimized nutritionfeeding tubes or specialized formulas when oral intake isnt enough.
- Regular monitoringtracking bloodpressure trends, heart rhythm, and metabolic health.
RealWorld Case Snapshot
Meet Maya, a 42yearold who was diagnosed at age 2. With a team that introduced nighttime BiPAP ventilation and a tailored diet plan, she now works as a graphic designer and enjoys hiking on weekends. Her story underscores that with modern care, FD doesnt have to be a lifeshortening sentence.
Treatment Options Today
Symptomatic Management
Because theres no cure yet, treatment focuses on easing the daily challenges:
- Respiratory supportCPAP or BiPAP machines for sleeprelated hypoventilation.
- Gastrointestinal therapiesprokinetic agents, antireflux medication, and, when needed, gastrostomy tubes.
- Physical therapystrengthening exercises to improve gait and reduce fall risk.
- Bloodpressure regulationfludrocortisone or midodrine during orthostatic episodes.
Emerging DiseaseModifying Approaches
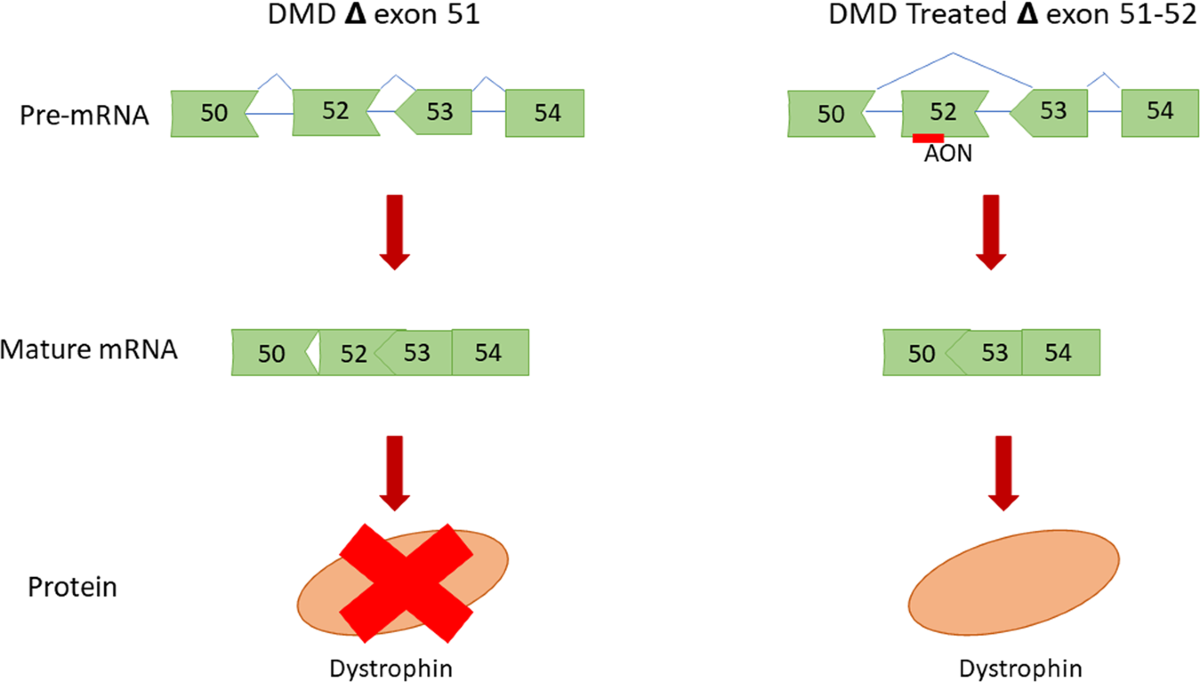
Researchers are hard at work on genetherapy and smallmolecule strategies that aim to boost the faulty ELP1 protein. A explored an antisense oligonucleotide designed to correct the splicing error caused by the common mutation. Early results are promising, showing modest improvements in autonomic function, though longterm data are still pending.
Treatment Decision Flowchart
Below is a handy mental flowchart you can walk through with your doctor:
- Is the patient experiencing respiratory symptoms?
Consider sleep studies Initiate CPAP/BiPAP. - Are feeding difficulties present?
Evaluate swallow study Add gastrostomy if needed. - Is bloodpressure instability an issue?
Trial fludrocortisone Adjust dosage based on response. - Is the patient eligible for a clinical trial?
Discuss experimental options with a specialist.
FD vs General Dysautonomia
Genetic vs Acquired Causes
While dysautonomia is an umbrella term for any autonomic dysfunction, familial dysautonomia is uniquely tied to a genetic mutation. General dysautonomia can stem from autoimmune disorders, diabetes, or even prolonged infections. In contrast, FD is present from birth due to the inherited ELP1 change.
Clinical Overlap & Key Distinguishing Signs
Both conditions may feature bloodpressure swings and gastrointestinal upset. However, a few telltale signs point more toward FD:
- Absence of tears in infants
- Earlyonset feeding problems
- Family history from Ashkenazi Jewish lineage
- Confirmed ELP1 mutation on genetic testing
SidebySide Comparison
| Feature | Familial Dysautonomia | General Dysautonomia |
|---|---|---|
| Cause | Inherited ELP1 mutation | Autoimmune, metabolic, etc. |
| Onset | Infancy | Any age |
| Tear production | Absent | Normal |
| Genetic test | Diagnostic | Usually not needed |
Managing FD in Adults
Transition of Care
Moving from pediatric to adult medicine can feel like switching tracks on a roller coaster. Its essential to find an adult neurologist or dysautonomia specialist who understands FDs lifelong nuances. A coordinated transfer plancomplete with a summary of past interventions, medication lists, and upcoming appointmentsmakes the shift smoother.
Lifestyle Adaptations
Living with FD isnt just about meds; its also about everyday tweaks:
- Work accommodationsflexible schedules for breathholding breaks, or the ability to work from home during flareups.
- Driving considerationssome adults may need adaptive controls or periodic medical clearance.
- Mental health supportcounseling or support groups can mitigate anxiety that often accompanies chronic illness.
Resources & Support Networks
Connecting with others who get it can be a lifesaver. The offers patient registries, research updates, and an online community where families share tips on everything from navigating insurance to cooking nutrientdense meals.
Conclusion
Weve walked through the essentials of familial dysautonomia as laid out in the trusted GeneReviews chapter: what it is, how it shows up, the genetics that drive it, testing pathways, treatment possibilities, and living well as an adult. Knowing the differences between FD and broader dysautonomia, understanding carrier risks, and staying informed about emerging therapies can empower you to make confident decisions. If anything sparked your curiosity or you have questions about your own situation, feel free to join the conversation in the comments or reach out to a genetic counselor. Together, we can turn a daunting diagnosis into a manageable, hopeful journey.
For families navigating treatment options and practical support, additional resources on related rare-disease assistance can help for example, information about patient support and insurance options is often key when planning long-term care. You can read more about Exondys 51 insurance and assistance for navigating coverage and support at Exondys 51 insurance and Exondys 51 assistance.