Quick Answers
What is supine hypertension? Its a rise in blood pressure that occurs when youre lying flat typically a reading of 140mmHg systolic or 90mmHg diastolic after youve been supine for at least five minutes.
Is it dangerous? Yes. Persistent high readings while lying down can increase the risk of stroke, heart failure, and make orthostatic hypotension (the dizzy feeling when you stand up) even worse.
How do doctors diagnose it? By measuring blood pressure in the supine position, then comparing those numbers to seated or standing readings. The ICD10 code for this condition is I95.1.
Understanding Causes
How It Happens: Core Pathophysiology
Imagine your bodys automatic brakes the baroreflex suddenly stop working. In many people with autonomic failure, that reflex is knocked out, so when you lie down the sympathetic nervous system goes into overdrive. Norepinephrine, renin, and angiotensin surge, pulling blood vessels tighter and pushing the pressure skyhigh. Thats the basic engine behind supine hypertension.
Whos at Risk?
About half of patients with neurogenic orthostatic hypotension (nOH) develop supine hypertension. The most common culprits are:
- Parkinsons disease
- Multiple system atrophy
- Diabetic autonomic neuropathy
- Older adults with chronic autonomic dysfunction
According to a review in , the prevalence in Parkinsons patients can reach 60%.
Key Symptoms to Spot
| Symptom | Typical Context |
|---|---|
| Morning headache or pressure feeling | After waking, while still lying down |
| Blurred vision or nausea | During acute spikes, often at night |
| Nighttime sweating, insomnia | BPrelated discomfort while supine |
| Worsening orthostatic dizziness during the day | Supineorthostatic hypertension syndrome |
These supine hypertension symptoms are often brushed aside as just a bad morning, but they can be clues that something deeper is happening.
RealWorld Example
John, a 68yearold man with Parkinsons, kept waking up with a throbbing headache. After a simple supine BP check, his numbers read 162/96mmHg lying flat versus 118/70mmHg seated. That single measurement turned his doctors attention to supine hypertension, leading to a treatment plan that dramatically reduced his morning misery.
Diagnosing Supine Hypertension
StepbyStep Measurement Protocol
1. Have the patient lie flat for five minutes in a quiet room.
2. Take the first blood pressure reading (use an automated cuff if possible).
3. Wait another five minutes, then take a second reading. Average the two if they differ by less than five mmHg.
4. Record seated and standing values for comparison.
This simple routine is enough to flag the condition, especially when paired with the ICD10 code I95.1 (supine hypertension ICD10).
When to Order Additional Tests
If the supine numbers are consistently above 180/110mmHg, or if the patient has other risk factors, consider:
- 24hour ambulatory blood pressure monitoring (ABPM) to capture nighttime trends.
- Laboratory workup: electrolytes, plasma norepinephrine, reninangiotensin levels.
- Imaging (renal artery Doppler, adrenal CT) if secondary causes like renal artery stenosis or pheochromocytoma are suspected.
Expert Insight Prompt
Dr. Laura Martinez, MD, Neurology, notes: A fiveminute supine hold is critical because a brief measurement can miss the delayed rise that characterizes true supine hypertension. (Source: .)
Treatment Options
Lifestyle First: Simple Tweaks
Before reaching for pills, try these lowrisk strategies:
- Headofbed elevation: Raise the mattress 1030 with wedges or blocks. This reduces the nocturnal pressure surge.
- Morning water bolus: Drinking 500ml of water can transiently raise standing pressure, balancing the daynight swing.
- Salt & fluid increase: If the kidneys can handle it, a modest boost in sodium and fluid can help keep pressures steadier.
These measures work especially well for the supine hypertension in pregnancy scenario, where medication options are limited and we want to keep both mom and baby safe.
Pharmacologic Toolbox
| Drug | Mechanism | Typical Dose (Supine) | When to Use |
|---|---|---|---|
| Midodrine | 1agonist vasoconstriction | 2.510mg PO q46h (avoid after 10pm) | Severe orthostatic hypotension with supine spikes |
| Pyridostigmine | Increases acetylcholine improves autonomic tone | 60mg PO q8h | Mildmoderate SH/OH, especially in Parkinsons |
| Clonidine (lowdose) | Central 2agonist reduces sympathetic outflow | 0.05mg PO nightly | When midodrine causes too high supine BP |
| Losartan | AngiotensinII receptor blocker | 2550mg PO nightly | Coexisting renal disease or high renin activity |
Each of these supine hypertension treatments has its own balance of benefits and risks. The midodrine story is a good illustration: while it lifts standing pressure, it can also push supine numbers higher, so we often pair it with a lowdose clonidine at night to blunt that effect.
DecisionTree Flowchart (Quick Visual)
Start Assess severity Try lifestyle changes first If supine BP 180/110mmHg, add lowdose clonidine If orthostatic symptoms persist, consider midodrine Recheck in 46weeks. This stepwise approach keeps patients safe while we finetune therapy.
Special Populations
Pregnancy
Data are sparse, so the mantra is nonpharm first. Elevating the head of the bed and staying wellhydrated are the mainstays. Any medication should be discussed with an obstetricianmaternalfetal medicine specialist.
Parkinsons Disease
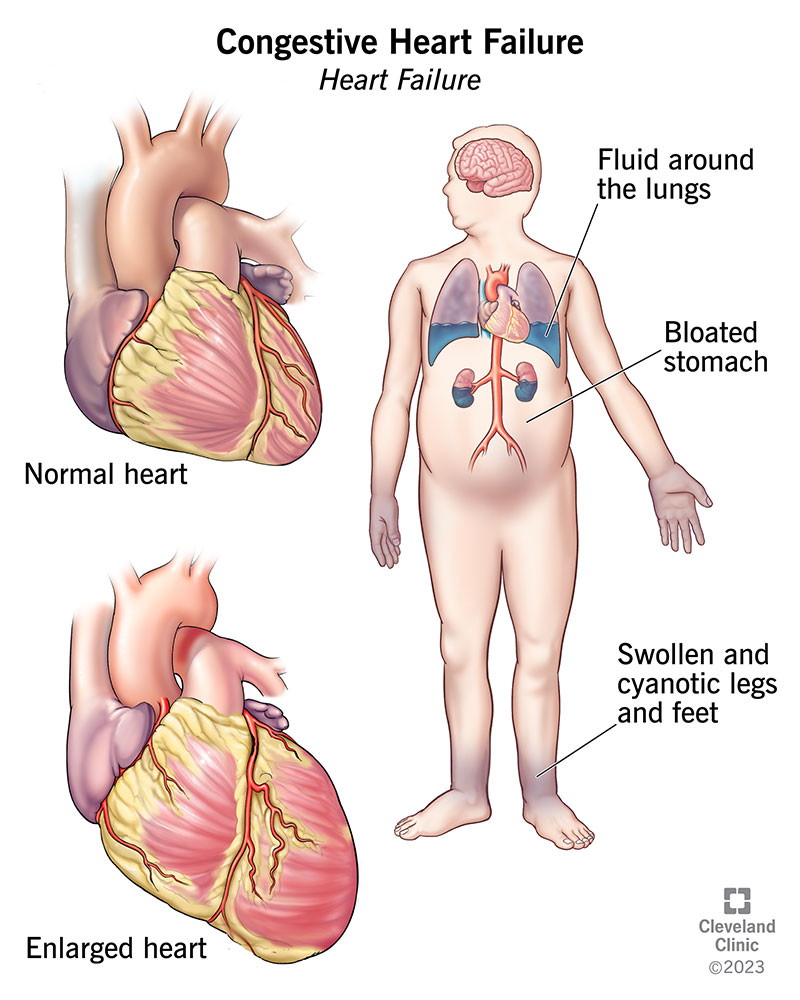
Midodrine can cause dramatic supine spikes in Parkinsons patients, so many clinicians start with pyridostigmine or a lowdose clonidine. Monitoring is key because the disease itself already messes with blood pressure regulation. For patients who also have heart-related symptoms such as swelling or shortness of breath, consider evaluating for heart failure and related issues like heart failure edema as part of the assessment.
Hospitalized Patients
In the ICU, isolated supine hypertension may appear after aggressive fluid resuscitation. The goal isnt to slam the numbers down to normal; a 1015% reduction usually suffices while avoiding hypotension when the patient sits up.
Monitoring & FollowUp
What to Track at Home
Give yourself a simple log:
- Morning supine BP (after waking, before getting up)
- Evening supine BP (before bedtime)
- Standing BP and any dizziness, lightheadedness, or headaches
- Medication doses and any sideeffects (e.g., swelling, dry mouth)
Having a paper or digital chart helps you see patterns and gives your doctor concrete data for adjustment.
When to ReEvaluate
Plan a checkin every 46weeks after any medication change. If you notice new symptomslike visual changes, sudden headaches, or swellingcall your provider sooner. Targetorgan damage (kidney, heart, retina) can develop silently, so regular labs and possibly an eye exam are wise.
Trusted Sources for Ongoing Learning
For the latest guidance, the American Heart Associations offers evidencebased recommendations on nocturnal hypertension. A 2022 cohort study in JAMA Cardiology linked persistent supine hypertension to a 30% increase in cardiovascular mortality, underscoring why we need to stay vigilant.
Conclusion
Supine hypertension may feel like an invisible foe, especially when youre already juggling orthostatic dizziness or a neurodegenerative condition. By measuring blood pressure correctly, recognizing the telltale morning headache or nighttime pressure surge, and applying a balanced mix of lifestyle tweaks and individualized medication, you can keep those numbers in check without sacrificing quality of life. Remember, the journey is personalwhat works for a patient with Parkinsons might need tweaking for a pregnant friend.
Wed love to hear your story. Have you tried headofbed elevation or a morning water bolus? What challenges have you faced with medication adjustments? Drop a comment below or reach out to your healthcare teamyoure not alone in navigating supine hypertension.
FAQs
What causes supine hypertension?
Supine hypertension occurs when the baroreflex fails, allowing sympathetic activity, norepinephrine, renin, and angiotensin to surge while lying flat, especially in autonomic failure and neurodegenerative diseases.
How is supine hypertension diagnosed?
Doctors measure blood pressure after the patient has been supine for at least five minutes, then compare it with seated and standing readings. Persistent readings ≥ 140/90 mmHg while lying down indicate the condition (ICD‑10 I95.1).
Can lifestyle changes help control supine hypertension?
Yes. Raising the head of the bed 10–30°, staying well‑hydrated, using a morning water bolus, and modestly increasing salt intake can lower nocturnal spikes without medication.
What medications are safest for treating supine hypertension?
Low‑dose clonidine at night, losartan, and pyridostigmine are commonly used. Midodrine can improve orthostatic hypotension but may raise supine pressures, so it’s often paired with a nighttime clonidine.
How does supine hypertension affect people with Parkinson’s disease?
Parkinson’s patients frequently experience exaggerated supine pressure surges. Clinicians often start with pyridostigmine or low‑dose clonidine and monitor closely, reserving midodrine for refractory orthostatic symptoms.