Balint syndrome is a rare neurological condition that messes with how the brain processes visualspatial information. It shows up as a classic triad optic ataxia, oculomotor apraxia, and simultagnosia and it usually stems from damage to both sides of the parietaloccipital area. If you or someone you love is facing these puzzling symptoms, youll want to know whats happening inside the brain, how doctors figure it out, and what can be done to improve daily life.
What Is the Triad?
Three core features
The hallmark of Balint syndrome is a set of three symptoms that often appear together:
- Optic ataxia difficulty reaching for objects under visual guidance, even though the muscles and eyes work fine.
- Oculomotor apraxia an inability to voluntarily shift gaze; the eyes seem stuck.
- Simultagnosia the brain can only recognize one object at a time, so a cluttered scene looks like a single spot.
Quicklook table: Triad vs. everyday examples
| Feature | Everyday analogy | Typical test |
|---|---|---|
| Optic ataxia | Missing a coffee mug when you try to grab it | Reachingforobjects task |
| Oculomotor apraxia | Can\'t look left or right on command | Saccadegeneration test |
| Simultagnosia | Seeing only one item on a crowded desk | Multipleobject visual search |
Seeing all three together is what makes neurologists say, Yep, thats Balint syndrome. It can feel like your brain has put on blinders you can see, but you cant see together.
Causes and Damage
Typical brain lesions
Balints syndrome is associated with damage to the dorsal visual stream, especially the parietaloccipital junction on both sides of the brain. The most common culprits are:
- Bilaterally symmetrical strokes, especially in the posterior cerebral artery territory.
- Traumatic brain injury that crushes the posterior lobes.
- Neoplastic growths (tumors) that press on both occipital lobes.
- Neurodegenerative conditions like posterior cortical atrophy (a variant of Alzheimers).
In short, anything that creates a double hit to the backupper part of the brain can set the stage for this syndrome.
Why bilateral?
The brains visualspatial processing relies on both hemispheres working together. When only one side is damaged, the other can often compensate. When both sides are knocked out, the system collapses, leading to the classic triad.
Brain Localization Areas
Key hotspots
The most reliable locations for Balint syndrome localisation are:
- Parietaloccipital junction (Brodmann areas 7&19).
- Superior parietal lobule, which helps coordinate handeye movements.
- Occipital cortex, where basic visual information is processed.
Illustrative diagram suggestion
When you write the full article, consider adding a simple brain sketch that shades the dorsal stream. A caption could note, Damage highlighted in red corresponds to the areas most often implicated in Balint syndrome, as described in recent neuroimaging reviews. Citing would bolster authority.
Diagnosis and Imaging
Helpful imaging studies
Radiology is a cornerstone of the workup:
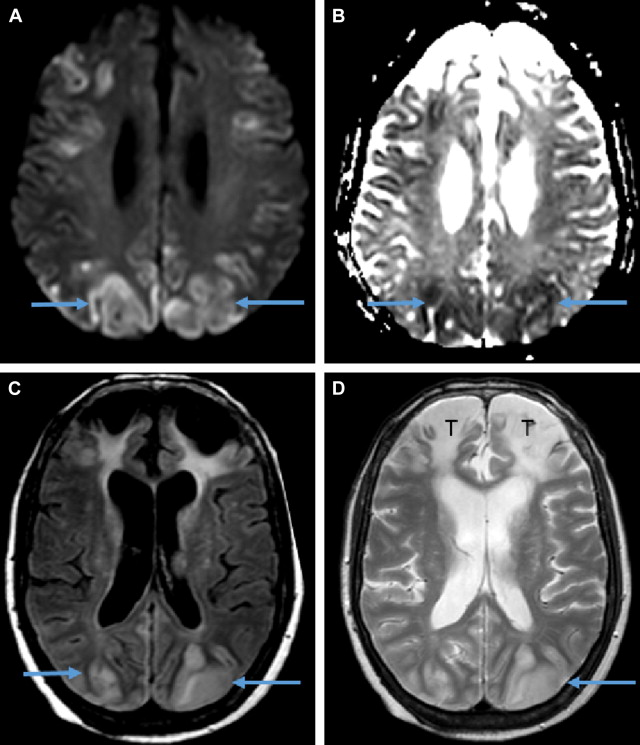
- MRI T2/FLAIR sequences reveal hyperintense lesions in the posterior regions; its the gold standard for spotting subtle bilateral damage.
- CT scan Quick to rule out acute hemorrhage, especially in emergency settings.
- Diffusiontensor imaging (DTI) Shows disrupted whitematter tracts in the dorsal stream, giving a deeper look at the connectivity loss.
Clinical bedside exams
Doctors also run a few simple tests to catch the triad:
- Saccadic eyemovement test The patient is asked to look quickly from one dot to another; hesitation signals oculomotor apraxia.
- Reachingforobject task A small object is placed on a table; misreaching suggests optic ataxia.
- Multipleobject identification The examiner shows a collage of pictures; the patient often names only one.
Diagnostic flowchart (suggested visual)
1 History & symptom check 2 Neurological exam 3 MRI/CT 4 Neuroophthalmology referral 5 Tailored rehab plan.
Treatment Options Overview
Rehabilitation first
Theres no magic pill that erases Balint syndrome, but intensive rehabilitation can make a world of difference. The main pillars are:
- Occupational therapy Drill reaching and objectmanipulation tasks to retrain optic ataxia.
- Vision therapy Saccade training and gazeholding exercises to improve oculomotor control.
- Cognitive strategies Teach patients to scan a scene systematically, reducing simultagnosias impact.
When surgery or meds matter
If an underlying tumor, abscess, or vascular malformation is discovered, neurosurgical removal or endovascular treatment becomes essential. For strokerelated cases, anticoagulation and bloodpressure management are standard, but they dont directly fix the visualspatial deficits.
Sample weekly rehab schedule
| Day | OT focus | Vision therapy | Home exercise |
|---|---|---|---|
| Mon | Reachtopoint drills | Saccade drills | 10min gazeholding |
| Wed | Bimanual coordination | Mirrorreading | 5min peripheral scanning |
| Fri | Realworld navigation | Simultaneous object identification | 15min cluttered tabletop task |
Related Neurological Conditions
Anton syndrome vs. Balint
Anton syndrome is sometimes confused with Balint because both involve visual processing problems. The key difference?
- Anton syndrome = cortical blindness with denial of vision (the patient insists they can see).
- Balint syndrome = preserved visual acuity but profound trouble integrating what is seen.
Other posteriorcortical disorders
Its useful to keep these on your radar, too:
- Posterior cortical atrophy (PCA) A gradual loss of visuospatial abilities, often mistaken for typical Alzheimers.
- Strabismic amblyopia Rarely mimics oculomotor apraxia, but usually shows up in childhood.
Comparison table: Balint vs. Anton vs. PCA
| Feature | Balint | Anton | PCA |
|---|---|---|---|
| Main symptom | Triad (optic ataxia, oculomotor apraxia, simultagnosia) | Denial of cortical blindness | Progressive visuospatial loss |
| Visual acuity | Normal | Severely reduced | Variable |
| Aware of deficit | Yes | No (confabulation) | Partial |
Pronunciation and Naming
How to say it correctly
Balint syndrome is pronounced /blnt sndrom/ think BALint SINdrohm. Youll sometimes see it written as Balints syndrome (with an apostrophe) because the condition is named after Hungarian neurologist RezsBlint. Most modern medical journals drop the apostrophe, so stick with Balint syndrome for consistency.
Living With Balint Syndrome
Imagine trying to navigate a grocery aisle where every product looks like a single dot, and reaching for an apple feels like trying to grab a ghost. Thats the daytoday reality for many patients. The good news? With early detection, targeted rehab, and a supportive team, people often regain enough function to live independently, drive with adaptive aids, and enjoy hobbies again.
Here are a few practical tips that weve heard work well:
- Clear the visual field. Keep your workspace tidy; fewer items mean less overload for simultagnosia.
- Use highcontrast objects. Brightly colored mugs, utensils, or phone chargers are easier to locate.
- Chunk tasks. Break complex actions (like dressing) into singlestep sequences and check off each one.
- Ask for help. A friend or caregiver can verbalize whats around you, reducing the pressure on your visual system.
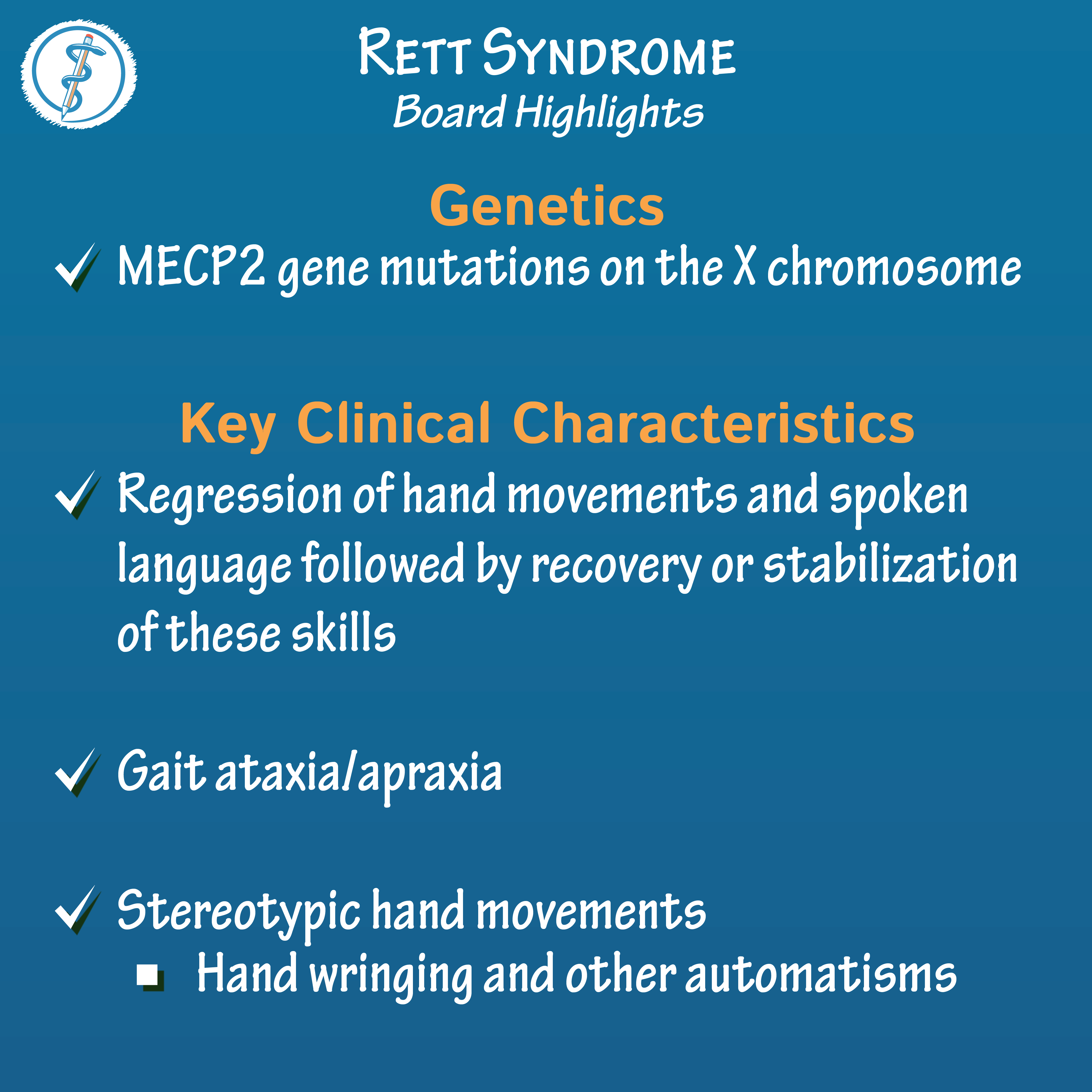
Remember, youre not alone. Support groupsboth inperson and onlineoffer stories from people whove turned the blind spot of Balint syndrome into a place of learning and growth. For families navigating complex care needs, resources that explain related conditions such as Rett syndrome criteria can sometimes be helpful for comparison when neurodevelopmental or degenerative patterns are being considered.
Conclusion
Balint syndrome may sound daunting, but understanding its triad, causes, and the brain regions involved helps demystify the condition. Diagnosis leans on careful clinical exams and modern imaging, while treatment focuses on multidisciplinary rehabilitation and addressing any underlying injury or disease. Though the syndrome can restrict everyday activities, many patients achieve meaningful improvements with early, personalized therapy. If you notice any of the symptomsespecially the odd combination of reaching errors, stuck eyes, and oneobjectatatime visiontalk to a neurologist or neuroophthalmologist right away. Staying informed, seeking help, and connecting with others can turn uncertainty into empowerment.
What experiences have you or a loved one had with visualspatial challenges? Share your thoughts in the comments, or drop a question if somethings unclearwere all in this learning journey together.
FAQs
What are the three core symptoms of Balint syndrome?
The syndrome is defined by a triad: optic ataxia (trouble reaching for objects under visual guidance), oculomotor apraxia (difficulty voluntarily moving the eyes), and simultagnosia (inability to perceive more than one object at a time).
Which brain areas are most commonly damaged in Balint syndrome?
Lesions typically involve the bilateral parietal‑occipital junction (Brodmann areas 7 & 19), the superior parietal lobule, and surrounding dorsal visual‑stream cortex.
How is Balint syndrome diagnosed?
Diagnosis combines bedside tests (saccadic eye‑movement, reaching‑for‑object, multiple‑object identification) with imaging such as MRI (gold standard), CT for acute bleed, and diffusion‑tensor imaging to assess white‑matter tract disruption.
Can Balint syndrome be treated?
There is no cure, but intensive multidisciplinary rehabilitation—occupational therapy, vision therapy, and cognitive strategies—can markedly improve daily functioning. Surgery or medication is only indicated when an underlying tumor, abscess, or vascular lesion is present.
How does Balint syndrome differ from Anton syndrome?
Balint syndrome patients have normal visual acuity but suffer from severe visuospatial integration problems. Anton syndrome involves cortical blindness with denial of vision, so the patient insists they can see despite being blind.