Quick Answer Section
Seeing a sudden headache, trouble balancing, or an unexpected seizure can feel like your body is sending an urgent SOS. If you or someone you love has leukemia, these neurological signs might mean the disease has entered the spinal fluida condition doctors call central nervous system (CNS) leukemia.
In short, the most common redflag symptoms are persistent headaches, nausea or vomiting that won't quit, vision changes, loss of balance, and new-onset seizures. If any of these pop up, call your oncologist todayearly testing can make a huge difference.
CNS Overview Basics
What does it mean when leukemia is in the spinal fluid?
Leukemia in the spinal fluid means that malignant white blood cell blasts have crossed the blood-brain barrier and are floating in the cerebrospinal fluid (CSF) that bathes the brain and spine. This is called CNS involvement. It can happen with both acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML), though it's a bit more common in ALL.
How do the cells get there?
Think of the blood-brain barrier as a highly secured castle wall. In some cases, leukemic cells find a secret tunnelthey slip through tiny gaps, hitch a ride with circulating blood, and settle in the meninges (the protective layers around the brain and spinal cord). High-risk genetic changes, a young age, or an aggressive disease course can increase the odds of this tunnel-finding behavior. In cases such as acute myeloid leukemia pregnancy, monitoring for neurological complications is especially important due to the dual risks to mother and child.
Symptom Checklist Overview
Neurological redflags
- Headaches: New or worsening headaches that don't respond to usual painkillers.
- Vision problems: Double vision, blurry sight, or sudden loss of peripheral vision.
- Balance loss: Feeling wobbly, stumbling, or difficulty walking in a straight line.
- Seizures: Any unexplained convulsion, even if it's just a brief blank-out.
- Mood changes: Uncharacteristic irritability, confusion, or personality shifts.
Gastrointestinal clues tied to CNS disease
- Nausea & vomiting: Persistent bouts that aren't linked to medication side-effects.
- Unexplained fatigue: A crushing tiredness that feels deeper than regular anemia.
Gender-specific notessymptoms of leukemia in females
Women may notice a mix of typical anemia fatigue plus menstrual irregularities that seem out of the blue. When these combine with any of the neurological signs above, it's a good idea to bring it up with the care teamthey'll often order a CSF test to be safe. If these findings arise during pregnancy, a tailored leukemia pregnancy treatment plan is essential to optimize maternal and fetal outcomes.
Diagnosis Process Steps
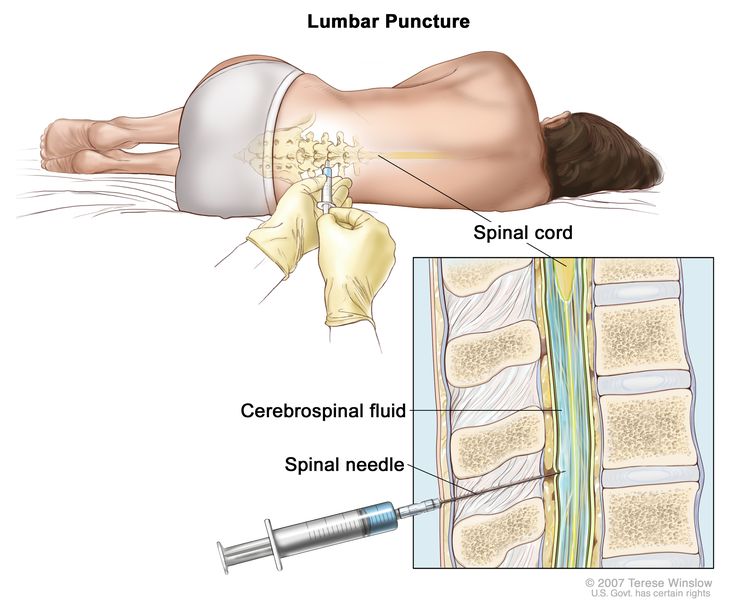
Lumbar puncture & CSF analysis
The gold-standard test is a lumbar puncture (spinal tap). A needle is gently inserted into the lower back to draw a small amount of CSF. The lab looks for:
- Leukemic blasts under the microscope.
- Flow cytometry patterns that match the blood leukemia.
- Molecular markers (PCR) that can predict response to therapy.
Doctors usually give a local anesthetic and a short period of rest afterward to reduce post-procedure headache.
Imaging studies
If a patient has focal neurological deficits, an MRI of the brain and spine can reveal masses, hydrocephalus, or areas of inflammation that need urgent attention.
Prognostic labs & survival stats
When we talk about AML pregnancy treatment outcomes, the numbers are sobering but not hopeless. For AML patients with CSF involvement, 2-year overall survival hovers around 3045%. In ALL, especially in children, the outlook improves to roughly 6070% when CNS-directed therapy is started early.
| Condition | 2-Year Survival | Key Prognostic Factor |
|---|---|---|
| AML with CSF positivity | 3045% | Blast count in CSF, age <30y |
| ALL with CNS involvement (children) | 6070% | Early intrathecal clearance |
| ALL with CNS involvement (adults) | 4055% | Presence of high-risk cytogenetics |
Treatment Options Guide
Intrathecal chemotherapy
Think of this as a direct-hit strategy. A tiny dose of chemotherapy (often methotrexate, cytarabine, and hydrocortisone) is injected straight into the CSF through a lumbar puncture or an Ommaya reservoir. This bypasses the blood-brain barrier and attacks the leukemic cells where they hide.
Systemic therapy adjustments
When CSF is positive, oncologists usually intensify the systemic regimenadding extra cycles or higher-dose agents that have better CNS penetration. For AML, high-dose cytarabine is a common choice; for ALL, a regimen like hyperCVAD may be altered.
Radiation & stem cell transplant
In refractory cases, cranial or craniospinal radiation can shrink meningeal disease, but it comes with long-term risks (cognitive decline, secondary cancers). Allogeneic stem cell transplant offers a chance at durable remission, especially for high-risk AML in the spinal fluid.
Emerging & clinical-trial options
Targeted therapies that can cross the blood-brain barrier (e.g., FLT3 inhibitors for FLT3-mutated AML, IDH1/2 inhibitors) are showing promise in early trials. Even CAR-T cell therapy, once adapted for CNS disease, might become a game-changer down the road.
Prognosis Outlook Summary
Survival numbers compared
The survival without prostate tends to be slightly higher than spinal fluid figures because solid brain lesions are rarer than meningeal spread. Still, early detection of spinal fluid involvement is the biggest lever you have to improve outcomes.
Monitoring after treatment
After induction therapy, most patients get a repeat lumbar puncture every 34 weeks until the CSF is clean. Then, surveillance usually switches to a schedule of every 3 months for the first year, then every 6 months. Long-term survivors are monitored for neurocognitive effects, endocrine issues, and secondary malignancies.
Real World Stories
Childhood casea brave little fighter
Eight-year-old Maya was diagnosed with ALL. Her parents thought the headaches were just school stress, until she started stumbling during recess. A quick lumbar puncture revealed blasts in her CSF. Within weeks, she began intrathecal methotrexate, and her headaches faded. Today, at age ten, Maya is thriving in school and loves drawing superheroesa reminder that early action can restore a bright future.
Adult journeybalancing work and treatment
Mark, a 32-year-old software engineer, had AML. After a routine checkup, he reported a new, persistent migraine. A CSF analysis showed involvement. He started an intensified chemo protocol and, while on sick leave, set up a home workspace to keep his projects alive. Support groups from the Leukemia & Lymphoma Society helped him stay motivated, and Mark now shares his story on a blog to help others navigate the same maze.
Bottom Line Tips
- Watch for headaches, vomiting, vision changes, balance loss, or seizuresthey're the loudest alarms.
- If any redflag appears, request a CSF test promptly; early diagnosis saves lives.
- Intrathecal chemotherapy is the cornerstone of treatment; don't skip it.
- Stay on a strict follow-up schedule; regular lumbar punctures catch relapse early.
- Lean on reputable resourcesHealthTree, the American Cancer Society, and patient-led advocacy groupsfor accurate information and emotional support.
Remember, you're not alone in this. Whether you're a parent, a partner, or the patient yourself, reaching out for help, asking questions, and staying informed are powerful moves. If you have thoughts, experiences, or questions, please share them in the commentstogether we can turn uncertainty into confidence.
Take care of yourself, stay vigilant, and keep hope alive. You've got this.
FAQs
What are the first signs of leukemia in spinal fluid?
Early warning signs include persistent headaches, nausea or vomiting, double vision, loss of balance, and new‑onset seizures.
How is CNS leukemia diagnosed?
The definitive test is a lumbar puncture to collect cerebrospinal fluid, which is then examined for leukemic blasts using microscopy, flow cytometry, and molecular PCR techniques.
What treatments are used for leukemia in the spinal fluid?
Intrathecal chemotherapy (e.g., methotrexate, cytarabine, hydrocortisone) is the cornerstone, often combined with intensified systemic therapy, radiation in refractory cases, and sometimes stem‑cell transplant.
Can leukemia in spinal fluid be prevented or caught early?
While it cannot always be prevented, regular monitoring—including scheduled CSF analyses during treatment—helps detect CNS involvement early, improving outcomes.
What follow‑up care is needed after treatment for CNS leukemia?
Patients typically have repeat lumbar punctures every 3‑4 weeks until CSF is clear, then routine checks every 3 months for the first year and every 6 months thereafter, with attention to neurocognitive and endocrine health.