Finding out you have AML while youre pregnant feels like the universe just pressed fastforward on a scary movie you never wanted to watch. Youre juggling a lifechanging diagnosis with the hopes, fears, and countless questions that come with a new baby on the way. Lets cut through the noise, get straight to the facts you need, and keep the conversation as warm and supportive as a friend whos been there.
Understanding AML
Acute Myeloid Leukemia (AML) is a fastgrowing cancer of the bloodforming cells in bone marrow. Those mischievous myeloblasts crowd out healthy blood cells, leading to fatigue, infections, bruising, and more. While its rareabout 1 in 75,000 pregnanciesits impact is huge, and early recognition is crucial.
One common worry is whether pregnancy can actually cause leukemia. shows no direct causal link; hormones and the immune shifts of pregnancy can mask early symptoms, making diagnosis trickier.
Spotting Signs Early
Because pregnancy already brings a lot of normal changes, distinguishing AML can feel like finding a needle in a haystack. Here are the red flags that deserve a closer look:
- Unexplained bruising or bleeding (gums, nose, or heavy periods)
- Persistent fatigue that doesnt improve with rest
- Night sweats and fever without infection
- Sudden weight loss or loss of appetite
- Abnormal blood counts on routine prenatal labs
If any of these show up, ask your OBGYN for a complete blood count (CBC) and a possible referral to a hematologist. Early testing is the first step toward a tailored AML pregnancy treatment plan.
Diagnostic Pathway
Once AML is suspected, doctors follow a clear, evidencebased pathwaymuch of it outlined in the latest and the British Society for Haematology leukemia in pregnancy guidelines. The process typically includes:
- Repeat CBC and peripheral smear
- Bone marrow aspirate (performed under local anesthesia)
- Cytogenetic and molecular testing to determine risk category
These results help doctors decide not only the intensity of treatment but also the safest timing relative to your trimester.
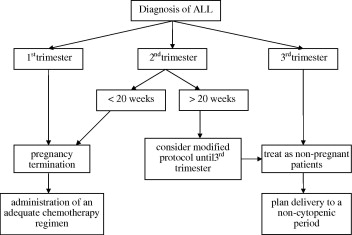
TrimesterSpecific Treatment
Now for the core of AML pregnancy treatment: what you can expect in each trimester. Think of it as a menu where the ingredients change depending on how far along you are.
| Trimester | Typical Regimen | Key Considerations | Fetal Outcome |
|---|---|---|---|
| First (013weeks) | Lowdose anthracycline alone or delayed induction | High teratogenic risk; often postpone intensive chemo until after 1213weeks | Risk of miscarriage; careful monitoring required |
| Second (1427weeks) | Cytarabine + daunorubicin (standard 7+3) | Maternal remission rates improve dramatically; fetal organogenesis largely complete | Low major malformation rates; increased neonatal monitoring |
| Third (28weeksbirth) | Continue standard induction; consider early delivery after 30weeks | Balancing maternal health with prematurity risks | Higher chance of healthy birth if delivered after 32weeks |
For a specific subtype called Acute Promyelocytic Leukemia (APML), the story shifts a bit. (alltrans retinoic acid) is safe in the second and third trimesters and can be lifesaving, but it demands vigilant monitoring for differentiation syndrome.
Balancing Benefits & Risks
Its natural to weigh the pros and cons like a scale of precious stones. On the benefit side, timely AML treatment boosts maternal fiveyear survival to around 55%, compared with less than 20% if therapy is delayed. On the risk side, the biggest concerns are:
- Potential teratogenic effects of chemotherapy in the first trimester
- Preterm birth if early delivery is chosen for maternal safety
- Longterm neurodevelopmental outcomes for the child
Heres a quick snapshot:
| Outcome | First Trimester | Second Trimester | Third Trimester |
|---|---|---|---|
| Maternal remission | 3040% | 7080% | 8590% |
| Fetal major malformations | 1520% | 25% | 13% |
| Live birth rate | 6070% | 8090% | 9095% |
These numbers are averages from large registry studies, so individual experiences can vary. Use them as a compass, not a crystal ball.
Supportive Care & Delivery Planning
Beyond chemo, supportive care keeps both you and the baby stable. Think hydration, infection prophylaxis, and managing tumor lysis syndromeall under the watchful eye of a multidisciplinary team (obgyn, hematologist, neonatologist, and a psychosocial counselor).
When it comes to delivery, timing is everything. If you achieve remission in the second trimester, many clinicians aim for a vaginal birth after 37weeks. If youre still fighting the disease late in the third trimester, a scheduled Csection at 3234weeks may be safer for the mother, followed by intensive neonatal care.
RealWorld Stories
Story time. Maya was 22 weeks pregnant when she got a shocking AML diagnosis. Her doctors started a standard 7+3 regimen, and after three cycles she was in complete remission. She carried her baby to 38 weeks, had a smooth vaginal delivery, and now both are thriving. Maya says the biggest thing that helped her was a clear, compassionate plan laid out by her care team.
In another case, Lenas AML was caught in the first trimester. Because the disease was highrisk, her hematologist recommended a brief delay of intensive chemo, followed by a lowdose anthracycline to buy time. At 14 weeks, she began full treatment, achieving remission by week 22, and delivered a healthy baby at 36 weeks via Csection. Both stories highlight how personalized AML pregnancy treatment can turn daunting odds into hopeful outcomes.
Answers to Common Questions
Can a woman with leukemia get pregnant? Absolutelymany women conceive after treatment, especially once theyre in remission. Fertility preservation (egg freezing or ovarian suppression) is often discussed before therapy starts.
Is ATRA safe in pregnancy? Lowdose ATRA is considered safe for APML after the first trimester, with careful monitoring for differentiation syndromea treatable complication.
What if Im already in my third trimester? The focus shifts to stabilizing the mother while planning the earliest safe delivery. Neonatal intensive care teams are ready to support preterm infants if needed.
Trusted Resources
When youre wading through medical jargon, these resources can be lifesavers:
- American Society of Hematology (ASH) How I Treat Leukemia in Pregnancy a clinicianwritten guide with uptodate evidence.
- British Society for Haematologys downloadable PDF with clear flowcharts.
- Leukaemia Foundations patientfocused pregnancy support pages practical tips for daily life.
- National Cancer Institutes pregnancycancer portal a reliable source for clinical trial options.
Moving Forward With Confidence
Facing AML while pregnant is a marathon, not a sprint. It demands courage, a solid support network, and uptodate medical guidance. The good news? With trimesterspecific AML pregnancy treatment, a coordinated care team, and informed decisionmaking, many mothers not only survivethey go on to watch their children grow.
Remember, youre not alone in this. Reach out to your healthcare providers, ask every question that pops into your mind, and lean on support groups who get the unique blend of hope and fear youre feeling. If you have a story to share or a question thats been nagging you, drop a comment below. Lets keep the conversation going, because together were stronger.
Take a deep breath. Youve got this.
FAQs
Is chemotherapy safe for the baby during pregnancy?
Chemo agents that are highly teratogenic are avoided in the first trimester. In the second and third trimesters, standard AML regimens (e.g., cytarabine + daunorubicin) have been used with low rates of major fetal malformations, though close monitoring is essential.
What symptoms should raise suspicion for AML while pregnant?
Look for unexplained bruising or bleeding, persistent fatigue, night sweats with fever, sudden weight loss, loss of appetite, or abnormal blood counts on routine prenatal labs. Any of these warrant a CBC and possible hematology referral.
How is AML treated if diagnosed in the first trimester?
Because organ formation is still occurring, doctors often use low‑dose anthracycline alone or delay intensive induction until after 12‑13 weeks. The goal is to balance maternal survival with minimizing teratogenic risk.
Can a mother breastfeed after completing AML treatment?
Most chemotherapy agents and targeted therapies are excreted in breast milk and are contraindicated while nursing. Women are usually advised to avoid breastfeeding for several weeks to months after the last dose, depending on the drug’s half‑life.
What fertility preservation options exist for women undergoing AML therapy?
Before starting treatment, options such as egg or embryo freezing, ovarian tissue cryopreservation, and ovarian suppression with GnRH agonists can be discussed with a reproductive specialist to improve future pregnancy chances.