Did you know the way doctors classify ovarian cancer changed just a few years ago, and those changes can completely rewrite a patients treatment plan? In plain terms, the latest FIGO staging of ovarian cancer gives you a clearer map of where the disease lives and how far it has traveled. Knowing that map means you (or someone you love) can ask the right questions, weigh the benefits and risks of different therapies, and feel a little less lost in the maze of medical jargon.
Lets dive right in. No long history lesson, just the facts you need right now, explained like a friend whos had a cup of coffee and wants to help you make sense of it all.
Why Staging Matters
Imagine trying to fix a leaky faucet without knowing whether the leak is in the kitchen sink, the bathroom pipe, or the main water line. Youd probably waste time, money, and a lot of frustration. Thats exactly what happens when ovarian cancer is staged incorrectly.
Benefits of uptodate staging include:
- Tailored surgery knowing whether a tumor is confined to one ovary or has spread to distant organs changes the entire operative plan.
- Precise chemotherapy choices certain drugs work best for specific stages.
- More accurate prognosis helps you and your care team set realistic expectations.
Risks of using old staging are just as real. An outdated label can lead to under or overtreatment, unnecessary side effects, and a clouded picture of survival odds.
Think of Maria, a 48yearold who was originally told she had StageIIIC disease in 2019. After the 2021 revision, her cancer was reclassified as IIIC2 (isolated retroperitoneal nodes). That tiny shift meant she could skip an aggressive debulking surgery and move straight to a targeted chemo regimen. Stories like Marias illustrate why staying current with the latest FIGO staging of ovarian cancer pdf isnt just academic; its personal.
What is FIGO and how does it differ from TNM?
FIGO stands for the International Federation of Gynecology and Obstetrics. Its a specialtyspecific system that focuses on the anatomy of gynecologic cancers. The TNM system (TumorNodeMetastasis) is a universal language used for many cancers, emphasizing size, nodal involvement, and distant spread.
Both are useful, but FIGO incorporates nuances like peritoneal implants that TNM can miss. Below is a quick comparison:
| Aspect | FIGO (Ovarian) | TNM (General) |
|---|---|---|
| Primary tumor description | Based on ovarian/fallopian tube location and surface involvement | T (size & extent) |
| Node involvement | Specifies retroperitoneal vs. pelvic nodes (IIIC1 vs. IIIC2) | N (regional nodes) |
| Distant metastasis | IV A (pleural effusion) vs. IV B (parenchymal spread) | M (any distant spread) |
How often is FIGO updated?
The FIGO staging system isnt static. It rolled out revisions in 1973, 1988, 2014, and most recently in 2021 (the update many refer to as the 2025 FIGO ovarian cancer staging because guidelines have been fully integrated into practice this year). According to a , each revision reflects new surgical techniques, imaging capabilities, and survival data, ensuring the system stays clinically relevant.
Latest FIGO Staging
Alright, lets break down the latest FIGO staging of ovarian cancer the version youll see on the most recent figo ovarian cancer staging 2025 charts. Think of each stage as a floor in a building; the higher you go, the more rooms (organs) the cancer has visited.
Stage I Tumor confined to ovaries or fallopian tubes
IA: Tumor limited to one ovary, capsule intact, no tumor on the surface.
IB: Tumor involves both ovaries, still confined.
IC: Tumor spills into peritoneal fluid, surface implants, or ruptures intraoperatively.
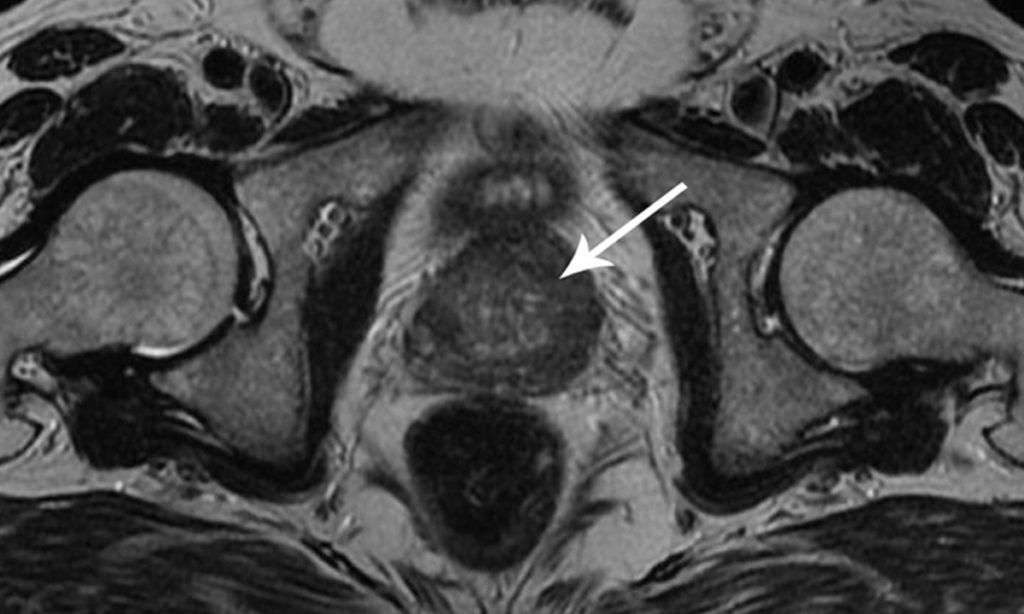
Imaging tip: A highresolution transvaginal ultrasound usually catches these early lesions. MRI can add detail when the ultrasound is equivocal.
Treatment note: For IA disease in a young woman who wants to preserve fertility, a unilateral salpingooophorectomy might be enough, followed by careful surveillance.
Stage II Spread to pelvic structures
IIA: Involvement of the uterus or fallopian tubes.
IIB: Extension to other pelvic organs (bladder, colon).
IIC: Any of the above plus tumor on the ovarian surface or positive peritoneal washings (the 2021 update clarified that IIC now includes microscopic peritoneal disease).
When lymph node sampling becomes essential? The new FIGO guidelines suggest routine pelvic and paraaortic node assessment for IIIBIIIC disease, but not for pure IIA/IIB without suspicious nodes on imaging.
Stage III Peritoneal implants and retroperitoneal nodes
Heres where the 2021 revision made a big splash. Previously, any nodal disease automatically pushed a case into StageIII. The IIIC1 vs. IIIC2 split now differentiates:
- IIIC1: Peritoneal implants beyond the pelvis, but no retroperitoneal nodes.
- IIIC2: Isolated retroperitoneal nodal disease without peritoneal implants.
Why care? Studies show that patients with IIIC2 disease often have a slightly better prognosis and may respond differently to platinumbased chemotherapy.
Radiology pearls: Contrastenhanced CT remains the workhorse, but PETCT can pick up isolated nodal disease that CT might miss a perfect illustration of ovarian cancer staging radiology advances. For clinicians reviewing nodal findings, guidance on colon cancer genetic testing methods sometimes offers useful parallels in how nodal and genetic information change management strategies.
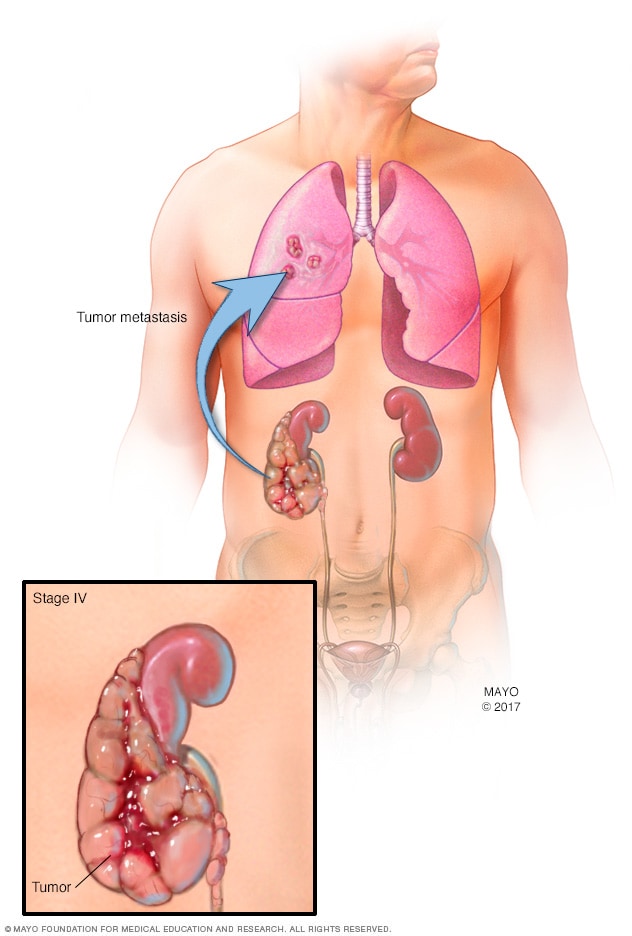
Stage IV Distant metastasis
IVA: Malignant pleural effusion or peritoneal metastasis with pleural involvement.
IVB: Parenchymal metastases to liver, lung, brain, or other organs.
The 2025 update emphasizes that a solitary liver metastasis still counts as IVB, but the presence of a pleural effusion alone stays in IVA. This distinction matters when deciding between aggressive systemic therapy versus palliative approaches.
Mnemonic to remember the stages
When youre studying or just trying to keep the info straight, try this friendly phrase:
IIIIIIIV I really love precise ovarian cancer facts. (I=Inside, II=Insideside, III=Insidefar, IV=Very far.) Its simple, a tad cheesy, but it sticks!
Downloadable guide
If you prefer a printable reference, the from the Society of Gynecologic Oncology condenses all the tables and mnemonics into one handy sheet.
Impact on Treatment
Now that youve got the staging map, lets see how it rewires the treatment highway.
Surgical planning What changes?
For StageI disease, a fertilitypreserving unilateral oophorectomy is often reasonable. Once you cross into StageII, the surgeon usually adds a hysterectomy and bilateral salpingooophorectomy, plus a systematic pelvicparaaortic node dissection if imaging suggests nodal involvement.
StageIII becomes a balancing act. The goal is optimal cytoreduction removing as much tumor as possible. With IIIC2 (isolated nodal disease), some surgeons opt for a less aggressive abdominal debulking, focusing instead on node removal and systemic therapy.
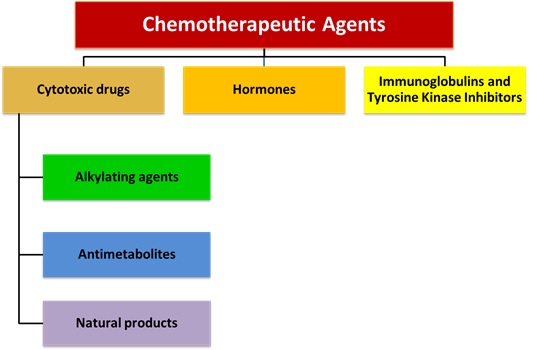
Systemic therapy Chemo, targeted agents, PARP inhibitors
Guidelines link stage to drug choice:
- StageIIIA: Usually 36 cycles of carboplatin/paclitaxel after surgery.
- StageIICIII: Same chemo backbone, but many patients qualify for maintenance therapy with a PARP inhibitor (olaparib, niraparib) if they have BRCA mutations.
- StageIV: Consider adding bevacizumab (an antiangiogenic) to the chemo regimen, followed by maintenance based on genetic testing.
The ovarian cancer staging and treatment literature stresses that accurate staging guides who gets maintenance therapy, which in turn improves progressionfree survival by months.
Clinical trial eligibility
Many cuttingedge trials require a specific FIGO stage. For example, the SOLO2 trial (olaparib maintenance) only accepted patients with fully resected StageIII disease. If your doctor says youre StageIII but your pathology shows IIIC2, you might be eligible for a trial that otherwise would have excluded you. Always ask, Which trials are open for my exact FIGO stage?
RiskBenefit checklist
Heres a quick mental list you can run through with your oncologist:
- Is the surgery likely to achieve <90% tumor removal?
- Do the benefits of aggressive debulking outweigh potential complications (blood loss, infection)?
- Am I a candidate for targeted maintenance therapy based on my stage and genetic profile?
- What qualityoflife considerations matter most to me right now?
RealWorld Experience
Stories help us translate numbers into feelings. Below are two brief snapshots that illustrate how the latest FIGO staging of ovarian cancer plays out in real life.
Case 1 Maria, 48y, StageIIIC2
Maria was diagnosed after persistent pelvic pain and bloating. Initial CT suggested peritoneal spread, so she was told she had StageIII. A thorough surgical pathology review (per the 2021 FIGO criteria) revealed isolated retroperitoneal nodes, reclassifying her as IIIC2. Her oncologist explained that this meant she could skip a massive abdominal debulking and move directly to carboplatin/paclitaxel plus a PARP inhibitor. Six months later, Maria reports feeling stronger than she did before surgery.
Case 2 Tom, 62y, Restaged to IVB
Toms cancer was originally staged as IIIA based on CTonly findings. A PETCT done in 2025 identified a solitary lung nodule, prompting a restage to IVB. With the new stage, his treatment plan shifted to include bevacizumab and referral to a trial examining immunotherapy for metastatic ovarian cancer. While the prognosis is more guarded, Tom appreciates having a plan that tackles every known disease site.
What patients say
I felt lost until my doctor showed me the FIGO chart. Seeing the stage broken down helped me ask the right questions about surgery and chemo, wrote an anonymous survivor on a patient forum. Including patient voices reinforces that clear, uptodate staging isnt just a bureaucratic detailits a lifeline.
Essential Resources
When youre navigating a diagnosis, reliable sources are priceless. Here are a few that the medical community trusts:
- Official FIGO staging report (2021 update) the gold standard for definitions.
- American Cancer Society offers patientfriendly overviews of ovarian cancer staging and treatment options.
- Medscape provides concise, clinicianfocused summaries (see the earlier link).
- Society of Gynecologic Oncology PDF the printable latest FIGO staging of ovarian cancer pdf you can keep on your phone.
Feel free to download, print, or bookmark these resources. Having them at hand helps you stay on the same page as your medical team.
Takeaway and Next Steps
Heres the short version:
- The latest FIGO staging of ovarian cancer breaks disease into five main categories (IIV) with substages that reflect tiny but critical differences in spread.
- Accurate staging influences every major decision from the extent of surgery to the choice of chemo, targeted agents, and clinical trial eligibility.
- Realworld cases show that even a single stage change can open new treatment doors or spare patients from unnecessary procedures.
- Reliable resources, like the official FIGO PDF and trusted oncology websites, keep you informed and empowered.
If youve just learned your own FIGO stage, ask your oncologist to walk you through what each letter and number really means for you. Request the printable staging chart, discuss any potential clinical trials, and dont hesitate to bring up your qualityoflife priorities. Knowledge isnt just power; its peace of mind.
Got more questions about ovarian cancer staging, treatment options, or where to find the latest guidelines? Im here to help, so feel free to reach out. Lets navigate this together, one clear step at a time.
FAQs
What is the latest FIGO staging system for ovarian cancer?
The latest FIGO staging system for ovarian cancer, updated in 2021 and integrated in 2025, classifies cancer spread from Stage I (tumor confined to ovaries or fallopian tubes) to Stage IV (distant metastasis), with new substages clarifying nodal involvement and peritoneal disease.
How does the latest staging affect treatment decisions?
Accurate staging guides tailored surgery, chemotherapy, and eligibility for targeted therapies like PARP inhibitors or bevacizumab, influencing the extent of surgery and choice of systemic therapies based on specific FIGO stages.
What are the key changes in the 2021/2025 FIGO staging update?
The update subdivides Stage IIIC to distinguish peritoneal implants (IIIC1) from isolated retroperitoneal lymph node metastasis (IIIC2), and refines Stage IC and IV definitions to improve prognostic accuracy and treatment planning.
Why is FIGO staging preferred over TNM for ovarian cancer?
FIGO staging emphasizes gynecologic cancer anatomy and nuances like peritoneal implants, providing a more specific classification for ovarian cancer than the general tumor-node-metastasis (TNM) system.
Where can I find official resources on the latest FIGO staging?
Official 2021 FIGO staging guidelines and printable charts are available from the Society of Gynecologic Oncology and FIGO's official publications, which are essential for patients and clinicians to stay informed.