Lets cut to the chase: the most effective medicines for chronic kidney disease (CKD) today are SGL2 inhibitors (think Farxiga), ACEinhibitors/ARBs, and the newer mineralcorticoid receptor blocker Finerenone. These drugs have solid proof of slowing kidney decline, lowering creatinine, and protecting your heart.
Why does this matter? Because picking the right pill (or combo of pills) is a balancing actmaximizing benefits while keeping sideeffects and drug interactions in check. Below well walk through the options, the science behind them, and practical tips to help you decide what works best for you.
Quick Check
When Do You Need Medication?
Typical red flags include persistent protein in the urine, a steady rise in serum creatinine, uncontrolled blood pressure, or an eGFR under 60mL/min/1.73m. The KDIGO 2024 guidelines suggest kicking off treatment as soon as these markers appear.
What Symptoms Should Prompt Action?
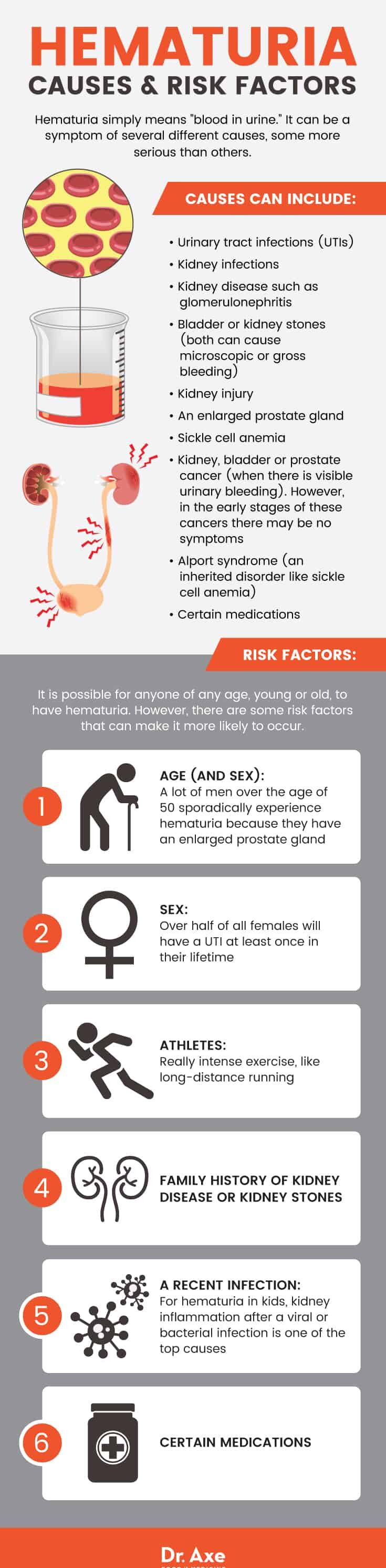
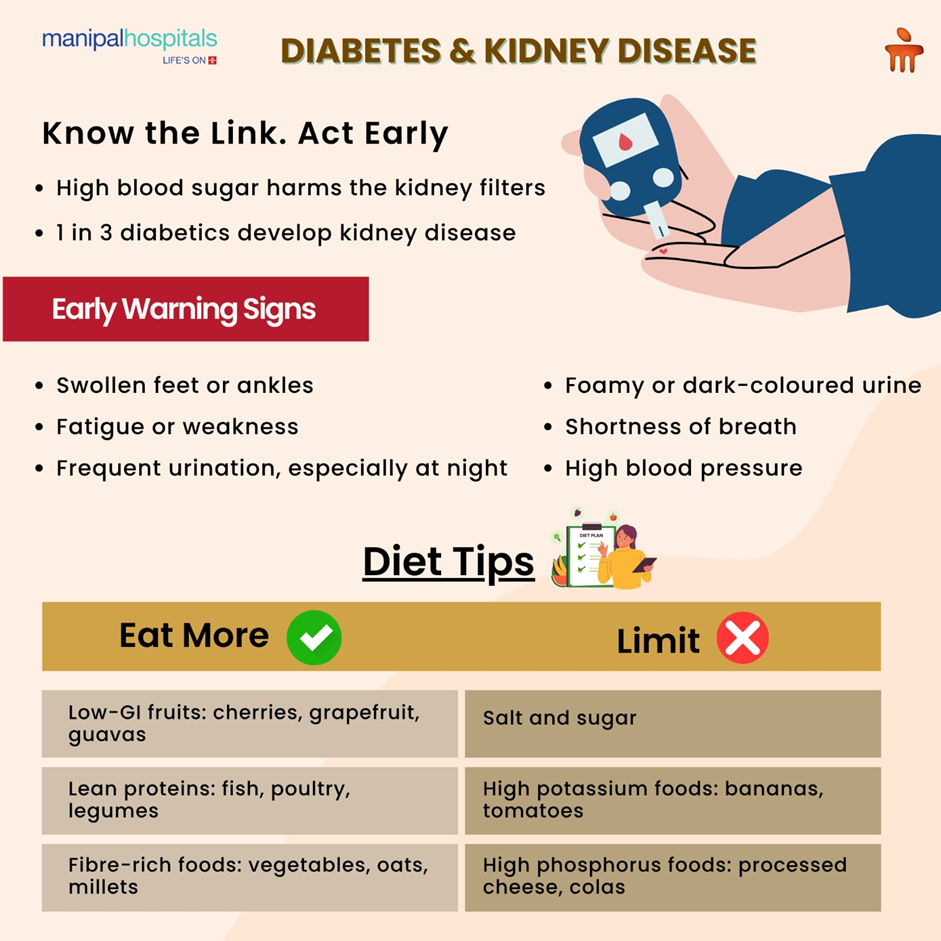
Swelling in ankles, fatigue, frequent urination, or a foggy feeling can all hint that your kidneys need a medical boost. If you spot any of these, its time to talk to a nephrologist.
RealWorld Snapshot
Maria, 58, was diagnosed at stage3 CKD after a routine blood test showed a creatinine of 1.8mg/dL. Within a month of starting an ACEinhibitor and adjusting her diet, her creatinine slipped to 1.5mg/dLproof that early treatment works.
Core Medications
| Medication Class | Brand (US) | How It Helps Kidneys | Key Study / Guideline |
|---|---|---|---|
| SGL2 inhibitors | Farxiga (dapagliflozin) | Reduces glomerular hyperfiltration, lowers albuminuria, slows CKD progression | |
| ACEI / ARB | Lisinopril, Losartan | Lowers blood pressure, reduces protein loss, blunts fibrosis | |
| Finerenone | Kerendia | Decreases albuminuria, offers cardiovascular protection | |
| GLP1 RAs | Ozempic (semaglutide) | Improves glycemic control; modest kidney benefit | |
| Statins | Atorvastatin | Reduces cardiovascular events, indirect kidney benefit | |
| Vitamin D & Calcium | Calcitriol, Calcium carbonate | Prevents bone loss, supports overall kidney health |
Why SGL2 Inhibitors Lead the Pack
These drugs were originally diabetes meds, but studies showed they also cut CKD progression by about 30% and lower the risk of heart failure. The most common sideeffects? Genital yeast infections and a modest dip in blood pressureboth manageable.
ACEI/ARB: The Classic Backbone
For decades theyve been the goto for anyone with proteinuria. They work by dilating the tiny blood vessels in the kidney, easing the pressure that can damage nephrons. Watch for hyperkalemia, especially if youre on a potassiumrich diet.
Finerenone: The New Kid on the Block
If you have diabetesrelated CKD, Finerenone can add an extra 15% risk reduction on top of an ACEI or ARB. Its not a firstline drug yet, but its gaining traction for patients who still progress despite standard therapy.
GLP1 RAs & Statins: Helpful Adjuncts
While they arent primary kidney protectors, they handle the big pictureblood sugar and heart healthwhich indirectly shields the kidneys.
Help Kidney Function
What Medications Help Kidney Function?
In a nutshell, the top five evidencebased drugs are:
- SGL2 inhibitors (dapagliflozin, empagliflozin)
- ACEinhibitors or ARBs (lisinopril, losartan)
- Finerenone
- GLP1 receptor agonists (semaglutide)
- Statins (atorvastatin)
These agents reduce protein loss, lower blood pressure, and tame inflammationkey drivers of kidney damage.
Best Medicine to Reduce Creatinine
Serum creatinine is a rough snapshot of how well your kidneys filter waste. SGL2 inhibitors and ACEI/ARBs consistently show the greatest drops, often pulling creatinine down by 0.20.4mg/dL within a few months.
Patient Story
John, 62, saw his creatinine tumble from 2.1mg/dL to 1.6mg/dL after adding Farxiga to his regimen while keeping his blood pressure under 130/80mmHg. He says he feels like his kidneys finally got a chance to breathe.
Drugs to Avoid
| # | Drug (Common Name) | Why It Hurts Kidneys | Safer Alternative |
|---|---|---|---|
| 1 | NSAIDs (ibuprofen, naproxen) | Can cause acute tubular necrosis and raise blood pressure | Acetaminophen (shortterm) |
| 2 | Gentamicin, Vancomycin | Nephrotoxic antibiotics that trigger interstitial nephritis | Adjusted dosing or alternative agents |
| 3 | Iodinated contrast agents | Contrastinduced nephropathy, especially in low eGFR | Isoosmolar contrast + hydration |
| 4 | Highdose loop diuretics (furosemide) | Excessive volume depletion stresses the kidneys | Lowdose thiazides (early CKD) |
| 5 | Herbal supplements with aristolochic acid | Direct tubular toxicity | Stick with physicianapproved botanicals |
| 6 | Syrianorange (Citrus aurantium) | Potentially raises blood pressure | Standard caffeine sources |
| 7 | Lithium | Chronic interstitial nephritis | Alternative mood stabilizers |
| 8 | Highphosphate phosphate binders | Can cause vascular calcification | Calciumbased binders when needed |
| 9 | Calcineurin inhibitors (cyclosporine) | Nephrotoxicity via vasoconstriction | Switch to safer immunosuppressants |
| 10 | Excessive caffeine | Can raise intraglomerular pressure | Moderate intake (200mg/day) |
Talking to Your Doctor
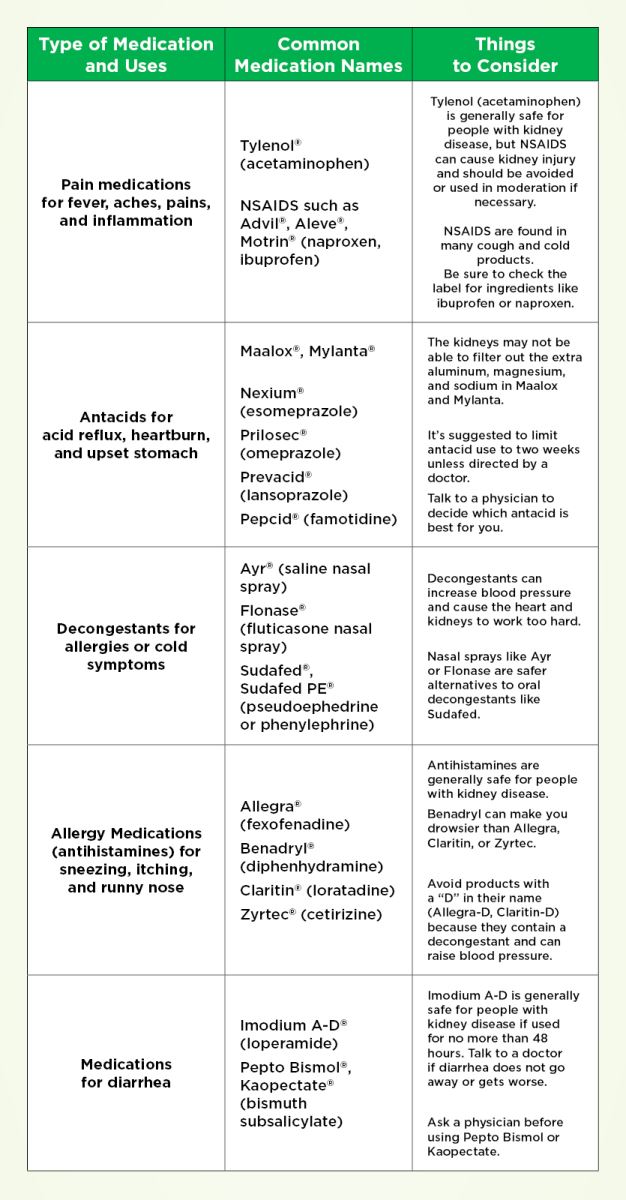
Never assume an overthecounter pill is harmless for CKD. Ask your provider for a renaladjusted dose, and keep an updated list of every medicationprescription, OTC, and supplement.
QuickCheck Worksheet
Downloadable PDFs (link in the sidebar of the original site) help you track risky drugs and note safer swaps. A simple table you can fill out at each doctors visit makes the conversation smoother.
Diet & Lifestyle
KidneyFriendly Diet Basics
Think low sodium (<2g/day), moderate protein (0.8g/kg body weight), and careful potassium monitoring if your labs call for it. Hydration is key, but avoid excessive fluids if youre on dialysis.
What Foods Help Repair Kidneys?
Research points to antioxidantrich choices: berries (especially blueberries), fatty fish (salmon, sardines), olive oil, garlic, and leafy greens like kale. These foods combat oxidative stressthe hidden enemy of kidney cells.
Sample 1Day Meal Plan
| Meal | What to Eat |
|---|---|
| Breakfast | Greek yogurt with fresh blueberries, a drizzle of honey, and a sprinkle of chia seeds |
| Lunch | Grilled salmon salad with mixed greens, cucumber, olive oillemon dressing |
| Snack | Apple slices with a tablespoon of almond butter |
| Dinner | Stirfried tofu, bell peppers, and broccoli in lowsodium soy sauce; serve over a small portion of brown rice |
| Evening | Herbal tea (chamomile) and a handful of unsalted walnuts |
DietMedication Interactions
If youre on calciumvitamin D combos, keep phosphate intake moderate. Highpotassium foods (e.g., bananas) might need to be limited if youre on an ACEI/ARB and your potassium spikes.
New Treatments
Latest Treatment for Chronic Kidney Disease
The wave of innovation right now includes dual GIP/GLP1 agonists like tirzepatide and nextgeneration SGL2 inhibitors such as sotagliflozin, which target both glucose and sodium reabsorption pathways.
New Drug Spotlight: Finerenone
Finerenone received FDA approval in 2022 after the FIGARODKD trial showed a 20% reduction in the composite outcome of kidney failure, sustained eGFR decline, or cardiovascular death. Its especially useful for patients who still progress on ACEI/ARB therapy.
Comparison: Finerenone vs. Traditional RAAS Blockers
| Feature | Finerenone | ACEI/ARB |
|---|---|---|
| Primary Action | Mineralcorticoid receptor antagonism | Angiotensin conversion inhibition / receptor blockade |
| Kidney Benefit | Albuminuria~30% | Albuminuria~20% |
| Cardio Benefit | Heart failure hospitalizations~15% | Hospitalizations~10% |
| SideEffects | Hyperkalemia (manage with diet) | Cough, hyperkalemia, angioedema |
| Cost (US) | $$$ (specialty drug) | $$ (generic widely available) |
Beyond Medication
When Medicine Isnt Enough
If CKD advances despite optimal drug therapy, the next steps are dialysis (hemodialysis or peritoneal) or transplantation. Both have lifechanging implications, so early discussion with a renal team is crucial.
Dialysis Basics
Hemodialysis is done at a center three times a week, while peritoneal dialysis can be performed at home, offering more flexibility but requiring strict hygiene.
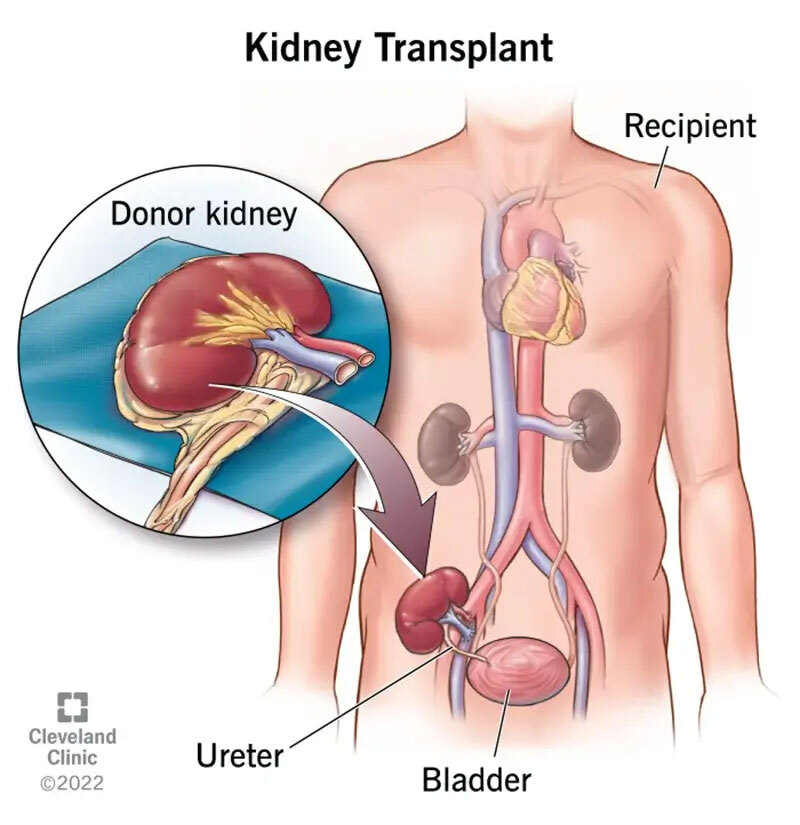
Kidney Transplant Overview
Eligibility hinges on cardiovascular health, absence of active infections, and a suitable donor match. Posttransplant, patients typically need lifelong lowdose immunosuppression, which introduces its own medication management challenges.
Choosing Your Medicine
Assess Personal Factors
Consider your CKD stage, presence of diabetes or hypertension, current meds, insurance coverage, and lifestyle preferences. A medication that works wonders for one person might be intolerable for another.
Shared DecisionMaking Checklist
- Identify your primary kidneyrelated goals (slow progression, lower creatinine, reduce blood pressure).
- Review each drugs benefits, sideeffects, and monitoring needs.
- Discuss cost and insurance coverage with your provider.
- Set a followup schedule for labs (eGFR, potassium, A1C).
- Ask for a written planeasy to reference at home.
Sample Conversation Starter
Doctor, I read that SGL2 inhibitors can lower my creatinine and protect my heart. Could we discuss whether starting Farxiga is right for me, and what monitoring youd recommend?
Conclusion
The best medicine for kidney disease isnt a single magic pillits a thoughtfully chosen combination of proven drugs (SGL2 inhibitors, ACEI/ARBs, Finerenone), a kidneyfriendly diet, and ongoing dialogue with your healthcare team. By balancing effectiveness with safety, you give your kidneys the strongest defense against further damage.
Ready to take the next step? Download our medication checklist, talk to your nephrologist about the options that fit your lifestyle, and stay tuned for updates on emerging therapies. Your kidneys deserve the best carelets give it to them together.
For readers managing related urinary or bladder symptoms in Parkinson's disease, resources on Parkinson OAB symptoms can help link kidney care with concurrent bladder issues.
FAQs
What medication classes are considered the best for kidney disease?
The most effective classes are SGL‑2 inhibitors, ACE‑I/ARBs, and the mineral‑corticoid receptor antagonist Finerenone, each backed by strong clinical trial data.
How do SGL‑2 inhibitors help protect the kidneys?
They reduce glomerular hyperfiltration, lower albuminuria, and slow chronic kidney disease progression by about 30%, while also offering cardiovascular benefits.
Can Finerenone be used together with an ACE‑I or ARB?
Yes. Finerenone is typically added on top of an ACE‑I or ARB in patients who continue to decline, providing an extra 15‑20% risk reduction for kidney outcomes.
What are the main side‑effects to watch for with these drugs?
SGL‑2 inhibitors may cause genital yeast infections and modest blood‑pressure drops; ACE‑I/ARBs can cause cough, hyperkalemia, or rare angioedema; Finerenone’s chief risk is hyperkalemia, manageable with diet and monitoring.
Are there any common medicines I should avoid with CKD?
Yes—NSAIDs, certain antibiotics like gentamicin, high‑dose loop diuretics, iodinated contrast agents, and herbal supplements containing aristolochic acid can worsen kidney function.