Cardiorenal syndrome (CRS) is a twoway street: when the heart falters, the kidneys can get hurt, and when the kidneys stumble, the heart can suffer. It can show up suddenly (acute) or creep in slowly (chronic), and the exact pattern depends on which organ started the trouble first.
Knowing the type of CRS, its underlying mechanisms, and the most uptodate treatments can mean the difference between vague fatigue and a clear plan that improves both survival and daily life. Below youll find a friendly walkthrough that covers everything you asked for from ICD10 codes to lifeexpectancy numbers in plain language and with a dash of personality.
What Is Cardiorenal Syndrome?
At its core, CRS is any acute or chronic problem in the heart or kidneys that could result in an acute or chronic problem in the other organ. In other words, the heart and kidneys talk to each other constantly, and when one of them sends a distress signal, the other often responds in kind.
Pathophysiology in a Nutshell
Think of the heart and kidneys as dance partners. When the hearts rhythm gets offbeat, blood backs up into the veins, raising pressure in the kidneys and squeezing them. Simultaneously, the body releases hormones (like reninangiotensinaldosterone) trying to compensate, but those hormones can also tighten blood vessels and worsen congestion. Add a pinch of inflammation and oxidative stress, and you have a perfect storm of organ crosstalk.
For a deeper dive, the outlines the neurohormonal loop, venous congestion, and immune activation in clear, clinicianfriendly language.
CRS Classification Types
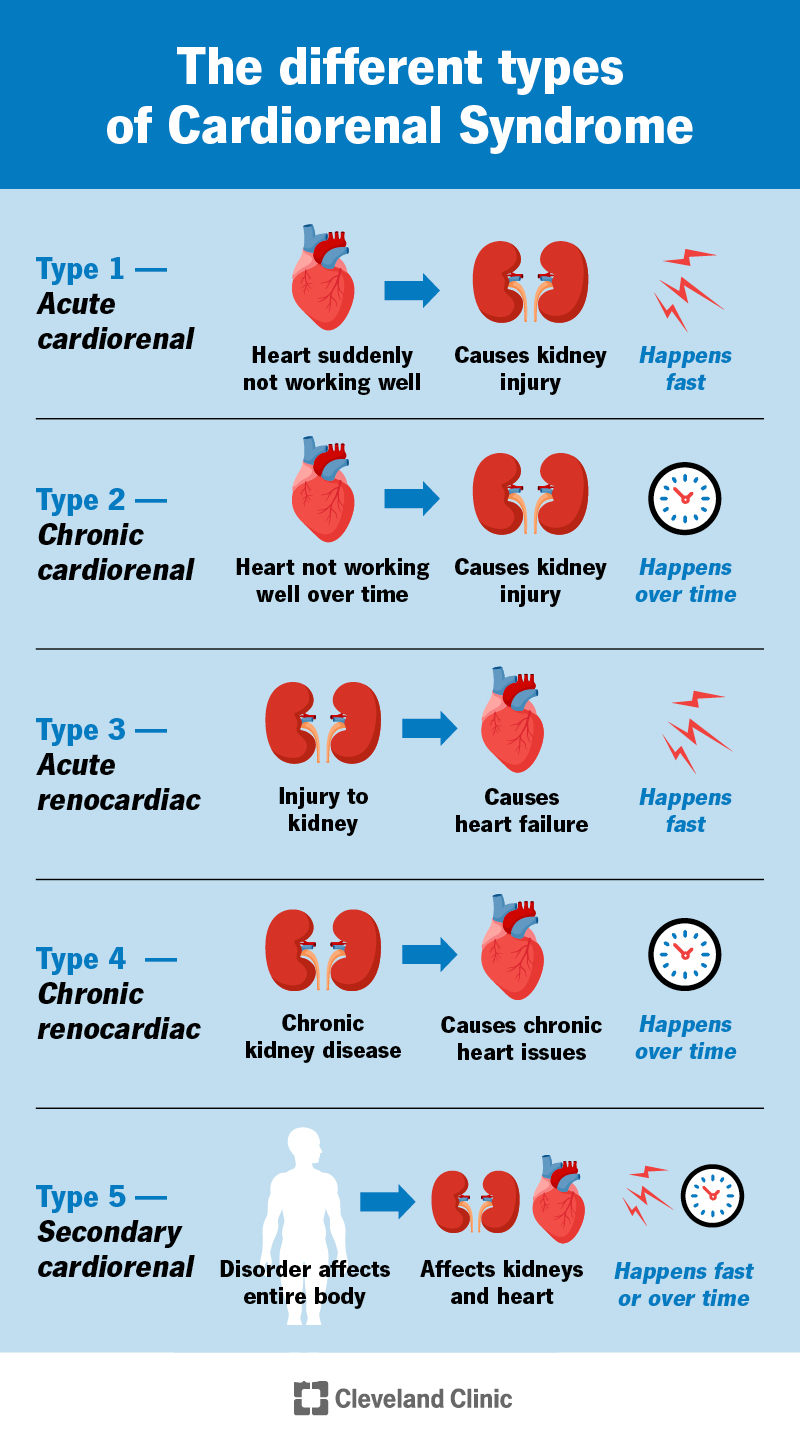
Experts usually split CRS into five types. Knowing the type helps you and your doctor decide which organ needs the most attention first.
| Type | Trigger Organ | Timeline | Typical Scenario |
|---|---|---|---|
| Type1 | Heart Kidney | Acute | Sudden heart failure leading to a rapid rise in creatinine. |
| Type2 | Heart Kidney | Chronic | Longstanding heart failure slowly worsening chronic kidney disease. |
| Type3 | Kidney Heart | Acute | Acute kidney injury (AKI) causing fluid overload and acute pulmonary edema. |
| Type4 | Kidney Heart | Chronic | Advanced CKD leading to leftventricular hypertrophy and heart failure. |
| Type5 | Both simultaneously | Either | Sepsis or systemic lupus triggering heart and kidney injury at the same time. |
The original classification was proposed by , and it remains the gold standard in both cardiology and nephrology circles.
Signs, Symptoms & Diagnosis
Because CRS is a blend of two organ failures, the symptoms can feel like a jumble of heart and kidney clues. Here are the most common red flags:
- Shortness of breath especially when lying down.
- Swelling in the ankles, feet, or abdomen (edema).
- Rapid weight gain due to fluid retention.
- Decreased urine output or a sudden change in urine color.
- Rising creatinine or BUN on labs.
- Elevated BNP or NTproBNP indicating cardiac stress.
Diagnostic Workup
When you walk into the clinic with those signs, your doctor will typically order a combo of blood tests, imaging, and sometimes hemodynamic monitoring:
- Blood panels: eGFR, creatinine, electrolytes, BNP/NTproBNP.
- Echocardiogram: evaluates heart function and pressures.
- Renal ultrasound: checks kidney size and blood flow.
- Chest Xray: looks for pulmonary congestion.
A practical flowchart goes like this: start with labs if creatinine spikes, order an echo if echo shows reduced ejection fraction, consider type1 or 2; if kidneys are the primary problem, look for type3 or 4. This stepbystep approach is echoed in the .
Risk Factors & Epidemiology
If youre wondering whos most likely to get CRS, think about the usual suspects for heart and kidney disease:
- High blood pressure
- Diabetes mellitus
- Existing chronic heart failure (NYHAIIIV)
- Chronic kidney disease (stage3 or higher)
- Older age, especially >65years
- AfricanAmerican ethnicity (higher prevalence of hypertensionrelated kidney damage)
Studies estimate that roughly 3040% of patients with chronic heart failure develop some degree of kidney dysfunction, and conversely, up to 25% of acute kidney injury cases are linked to acute heart failure. Those numbers come from a 2022 metaanalysis in Circulation that pooled data from more than 30,000 participants.
Treatment Options Overview
The goal of treatment is simple: fix the sick organ while protecting the healthy one. Below is a quick menu of what doctors typically consider.
Pharmacologic Therapy
- ACE inhibitors / ARBs / ARNIs: lower blood pressure, reduce afterload, and have proven kidneyprotective effects.
- SGLT2 inhibitors (e.g., dapagliflozin, empagliflozin): originally diabetes drugs, they now shine in both heart failure and CKD. A 2023 trial showed a 10% reduction in mortality for CRS patients on dapagliflozin.
- Mineralocorticoid receptor antagonists: help control fluid overload but need close monitoring of potassium.
- Loop diuretics: the workhorse for congestion; doseadjust based on kidney response.
Device & Procedural Options
- Ultrafiltration: mechanically removes excess fluid when diuretics fail useful in type1 CRS.
- Cardiac Resynchronization Therapy (CRT): can improve heart function, indirectly easing kidney stress.
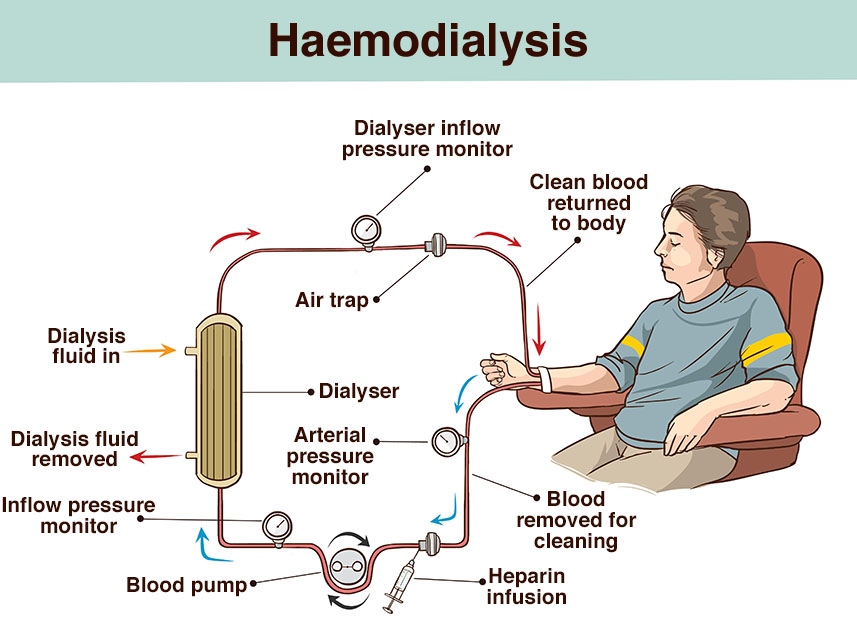
- Renal replacement therapy (dialysis): reserved for severe AKI or endstage CKD when other measures dont work.
Lifestyle & SelfCare
Even the best meds cant replace good habits. Here are three things that make a real difference:
- Salt restriction: aim for <2g per day (about a teaspoon).
- Fluid management: many doctors recommend <2L of fluid daily, but individual limits vary.
- Regular aerobic activity: short walks or gentle cycling help keep both heart and kidneys happy.
Prognosis and Life Expectancy
Lets be honest: CRS is serious. The fiveyear mortality hovers around 4555%, depending on the type and how early treatment starts. However, hope isnt lost. Patients who receive early SGLT2 inhibition, optimal bloodpressure control, and careful diuretic titration can see a measurable survival bump.
Key factors that tip the scales in your favor include:
- Higher baseline eGFR (better kidney reserve).
- Lower NYHA class (milder heart failure).
- Absence of diabetes or severe hypertension.
- Adherence to medication and lifestyle recommendations.
A graphical survival curve from a 2023 Kidney International cohort shows that patients on combined ACEI and SGLT2 therapy have a roughly 12% higher 3year survival than those on ACEI alone.
ICD10 Coding Guide
Accurate coding helps ensure you get the right reimbursement and that your medical record truly reflects the complexity of CRS. Heres a quick cheatsheet:
- Primary code:
I51.9Cardiovascular disease, unspecified is often used when CRS is the main concern. - Secondary kidney codes:
N18.9(CKD, unspecified) orN17.9(AKI, unspecified), depending on acuity. - Heartfailure code:
I50.9(Heart failure, unspecified) for chronic presentations.
When documenting, be explicit: Patient presents with Type2 cardiorenal syndrome, chronic heart failure (I50.9) leading to CKD stage3 (N18.3). Clear language satisfies both clinicians and auditors, as highlighted in the .
Resources & Further Reading
If you want to dig deeper, these sources are reliable and written for both professionals and patients:
- (a solid starter).
- comprehensive classification and pathophysiology.
- easytoread symptom checklist.
- Download a free (youll need to replace the URL with your own file when publishing).
Conclusion
Cardiorenal syndrome sits at the crossroads of heart and kidney health, and understanding its type, underlying mechanisms, and evidencebased treatments is essential for anyone facing this complex condition. By recognizing early warning signs, using the right diagnostic tools, and adopting a balanced therapeutic strategyincluding the newest SGLT2 inhibitorsyou can markedly improve both survival and daytoday quality of life.
Keep the ICD10 codes handy for accurate documentation, stay updated with the latest guidelines, and dont hesitate to discuss personalized care plans with a cardiologynephrology team. If you found this guide helpful, feel free to share your thoughts, ask questions in the comments, or download our free cheatsheet to keep close at hand. Together we can navigate CRS with confidence and compassion.
FAQs
What are the five types of cardiorenal syndrome?
The five types are classified by which organ initiates the problem and whether it develops acutely or chronically: Type 1 (acute heart → kidney), Type 2 (chronic heart → kidney), Type 3 (acute kidney → heart), Type 4 (chronic kidney → heart), and Type 5 (both organs injured simultaneously).
How do I know if my symptoms are due to cardiorenal syndrome?
Common red flags include shortness of breath, swelling in the legs or abdomen, rapid weight gain, reduced urine output, rising creatinine or BUN, and elevated BNP/NT‑proBNP. Laboratory tests and imaging (echo, renal ultrasound, chest X‑ray) help confirm the diagnosis.
Which medications are most effective for treating CRS?
Guideline‑directed therapy includes ACE inhibitors/ARBs/ARNIs, SGLT2 inhibitors (e.g., dapagliflozin, empagliflozin), mineralocorticoid receptor antagonists, and loop diuretics. These agents improve both cardiac function and kidney outcomes when used appropriately.
When is ultrafiltration or dialysis needed?
Ultrafiltration is considered when severe fluid overload does not respond to high‑dose diuretics, especially in Type 1 CRS. Dialysis (hemodialysis or peritoneal) is reserved for refractory acute kidney injury or end‑stage chronic kidney disease when other measures fail.
What is the typical prognosis for someone with cardiorenal syndrome?
Five‑year mortality ranges from 45‑55 % overall, but early use of SGLT2 inhibitors, optimal blood‑pressure control, and diligent diuretic management can improve survival by about 10‑12 % over three years.