Lets cut to the chase: if you have type2 diabetes and your kidneys are sending SOS signals, the standout players right now are finerenone (KERENDIA) and the class of SGLT2 inhibitorsthink dapagliflozin. Together they can slow kidney decline, lower heartfailure risk, and keep you feeling more like yourself. Below, Ill walk you through why kidney health matters, which drugs truly help, how to choose the right combo, and what to watch out for, all in a friendly, nojargon style.
Why Kidney Matters
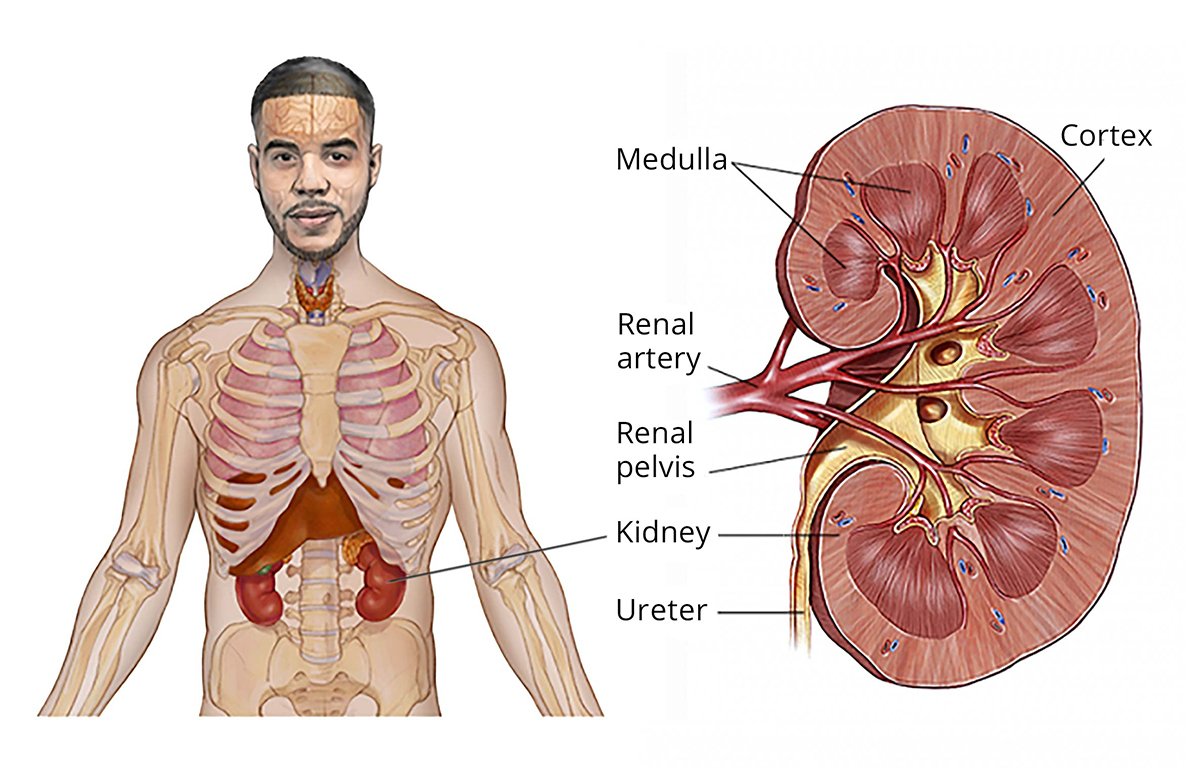
Kidney disease is the silent sidekick that shows up in up to 40% of people with type2 diabetes. Its not just a number on a lab report; it affects energy, blood pressure, and even mood. In simple terms, your kidneys filter waste and balance fluids. When diabetes spikes blood sugar, it can damage tiny blood vessels in the kidneys, leading to a cascade of inflammation and scarring. The good news? Modern medicines can intervene early enough to keep the decline at bay.
How Diabetes Damages the Kidneys
Think of your kidneys as a coffee filter. Hyperglycemia makes the filter pores swell (hyperfiltration), then the filter gets clogged with protein (albuminuria) and eventually tears. Over years, this turns into chronic kidney disease (CKD). According to the , more than 90% of adults with longstanding diabetes develop at least mild CKDso the stakes are high.
RealWorld Example
Meet Maria, 58, who discovered her eGFR had slipped to 45mL/min during an annual checkup. She felt fine, but her doctor warned her that without proper treatment, she could slide into stage3 CKD within a couple of years. Marias story illustrates how quickly quiet kidney damage can become a pressing health issue.
Core Kidney Drugs
When it comes to protecting kidneys in diabetes, a few drugs stand out for solid evidence and realworld success. Lets break them down, one by one.
Finerenone (KERENDIA) The New Kid on the Block
Finerenone is a mineralocorticoid receptor antagonist that reduces inflammation and fibrosis in the kidneys. The pivotal showed a 30% reduction in the composite outcome of kidney failure, sustained eGFR decline, or cardiovascular death among patients already on ACEI or ARB therapy.
Quick Answer (FeaturedSnippet Style)
Q: Which diabetes drug is best for diabetics with kidney disease?
A: Finerenone combined with an SGLT2 inhibitor (e.g., dapagliflozin) currently offers the strongest evidence for slowing CKD progression in type2 diabetes.
Safety & Monitoring
- Watch serum potassiumhyperkalemia occurs in ~5% of patients.
- Do not start if eGFR<25mL/min without specialist supervision.
- Baseline labs, then repeat at 4weeks and every 36months.
Expert Insight Prompt
Consider quoting a nephrologist, such as Dr.Luis Hernandez, who often says, Finerenone shines when paired with a reliable SGLT2 inhibitor; together they target both hemodynamic stress and inflammatory pathways.
SGLT2 Inhibitors dapagliflozin, empagliflozin, and Friends
SGLT2 inhibitors work by blocking glucose reabsorption in the kidney, which also reduces intraglomerular pressurea key driver of CKD. The FDA now approves dapagliflozin for CKD down to an eGFR of 20mL/min, making it a goto option even in fairly advanced disease.
Comparison Table Dapagliflozin vs. Empagliflozin vs. Sotagliflozin
| Drug | FDA CKD Indication | Typical Dose | Renal Outcome HR | Common SideEffects |
|---|---|---|---|---|
| Dapagliflozin | CKD 20mL/min | 10mg daily | 0.78 (renal) | UTIs, genital infections |
| Empagliflozin | CKD 20mL/min | 10mg daily | 0.80 (cardiovascular) | Dehydration, hypotension |
| Sotagliflozin | CKD 30mL/min (2025 FDA update) | 200mg BID | 0.74 (renal) | Dysgeusia, GI upset |
Patient Story
Carlos, 62, added dapagliflozin after his nephrologist noted a rising albumintocreatinine ratio. Within a year, his eGFR improved from 3844mL/min and his ACR dropped by 35%. It felt like the kidneys got a fresh coat of paint, he jokes.
GLP1 Receptor Agonists Adding a HeartKidney Duo
GLP1 RAs such as liraglutide and semaglutide are primarily bloodsugar and weightloss agents, but they also deliver modest kidney benefits (10% reduction in albuminuria). Theyre not the miracle drug for kidney disease, but theyre a solid addition if cardiovascular risk is high.
Traditional Diabetes Medicines That Can Hurt Kidneys
Not all diabetes meds are kidneyfriendly. Lets keep the conversation honest.
| Drug | Why It Can Be Risky for CKD | Practical Tip |
|---|---|---|
| Metformin (eGFR<30) | Risk of lactic acidosis | Hold if <30mL/min; reduce dose 3045mL/min |
| Sulfonylureas | Longer halflife hypoglycemia | Prefer shortacting agents (e.g., glimepiride) |
| Highdose ACEi/ARB alone | Hyperkalemia, especially with low eGFR | Combine carefully with finerenone or monitor potassium |
These examples answer the query diabetes medicine bad for kidneys and help you avoid the top10 drugs that cause kidney damage when other options exist.
Choosing the Right DiabetesKidney Drug
Picking the best combo isnt a onesizefitsall decision. It starts with understanding your kidney function.
Assess Your Kidney Function First
Ask your doctor for two key numbers:
- eGFR estimates filtration rate; the higher, the better.
- AlbumintoCreatinine Ratio (ACR) tells whether protein is leaking.
Guidelines suggest an ACR30mg/g or eGFR<60mL/min signals CKD that warrants kidneyprotective therapy.
Build a KidneyFriendly Regimen
Heres a straightforward threestep approach that many specialists follow:
- Baseline RAAS blockade ACEI or ARB to lower intraglomerular pressure.
- Add finerenone if albuminuria persists despite step1.
- Layer an SGLT2 inhibitor (dapagliflozin is a popular choice) unless contraindicated.
Practical DecisionTree (Visual Aid)
Imagine a flowchart:
- eGFR30mL/min? Yes Start SGLT2 inhibitor.
- Albuminuria30mg/g? Yes Add finerenone.
- Monitor labs every 36months; if potassium >5.5mmol/L, adjust finerenone dose.
Monitoring Checklist
- Serum potassium (baseline, 4weeks, then quarterly).
- eGFR and ACR (every 36months).
- Blood pressure (target <130/80mmHg).
- Signs of urinary or genital infection (especially on SGLT2 inhibitors).
When to Switch or Stop
If you experience severe hyperkalemia, recurrent UTIs, or persistent low blood pressure, talk to your provider about adjusting the regimen. Never stop a medication abruptly without a plan.
Balancing Benefits & Risks The Bottom Line
Summing it up:
- Finerenone cuts CKD progression risk by roughly 30% and works well alongside RAAS blockers.
- SGLT2 inhibitors (especially dapagliflozin) add another 2030% risk reduction and are safe down to an eGFR of 20mL/min.
- Both drugs have manageable sideeffectsmonitor potassium for finerenone and stay hydrated for SGLT2 inhibitors.
- Traditional agents like highdose metformin or sulfonylureas can be problematic when kidney function declines.
Bottom line: theres no single miracle drug for kidney disease, but the combination of finerenone and an SGLT2 inhibitor is the most powerful duo backed by current research. Together they protect your kidneys, lower heartfailure risk, and let you keep living the life you love.
Take Action Today
If youve been reading this because you or a loved one are navigating diabetes and kidney concerns, heres a simple next step:
- Schedule a bloodwork checkup to get your latest eGFR and ACR.
- Bring this article (or copy the key points) to your appointment and ask about finerenone and dapagliflozin as part of your treatment plan.
- Keep a medication diarynote any sideeffects, blood pressure changes, or new symptoms. Sharing this with your doctor makes finetuning easier.
Got questions or personal experiences youd like to share? Drop a comment below. Were all in this together, and your story might be the spark someone else needs to take action.
FAQs
What is the most effective diabetes kidney drug currently available?
Finerenone, especially when combined with an SGLT2 inhibitor like dapagliflozin, offers the strongest evidence for slowing CKD progression in type 2 diabetes.
Can I take an SGLT2 inhibitor if my eGFR is below 30 mL/min?
Yes. Dapagliflozin is FDA‑approved for CKD down to an eGFR of 20 mL/min, but you should be monitored closely by a nephrologist.
What are the main side‑effects of finerenone?
The most common safety concern is hyper‑kalemia (elevated potassium). Routine labs at baseline, 4 weeks, and then every 3‑6 months help manage this risk.
Do traditional diabetes medicines like metformin harm the kidneys?
Metformin is safe when eGFR is ≥30 mL/min, but should be reduced or stopped below that level due to lactic acidosis risk. Other agents such as sulfonylureas can cause hypoglycemia in CKD.
How should I monitor my kidney health while on these medications?
Track serum potassium, eGFR, and albumin‑to‑creatinine ratio every 3‑6 months, keep blood pressure <130/80 mmHg, and report any urinary infections promptly.