FAQs
What is the primary treatment for renal tubular acidosis?
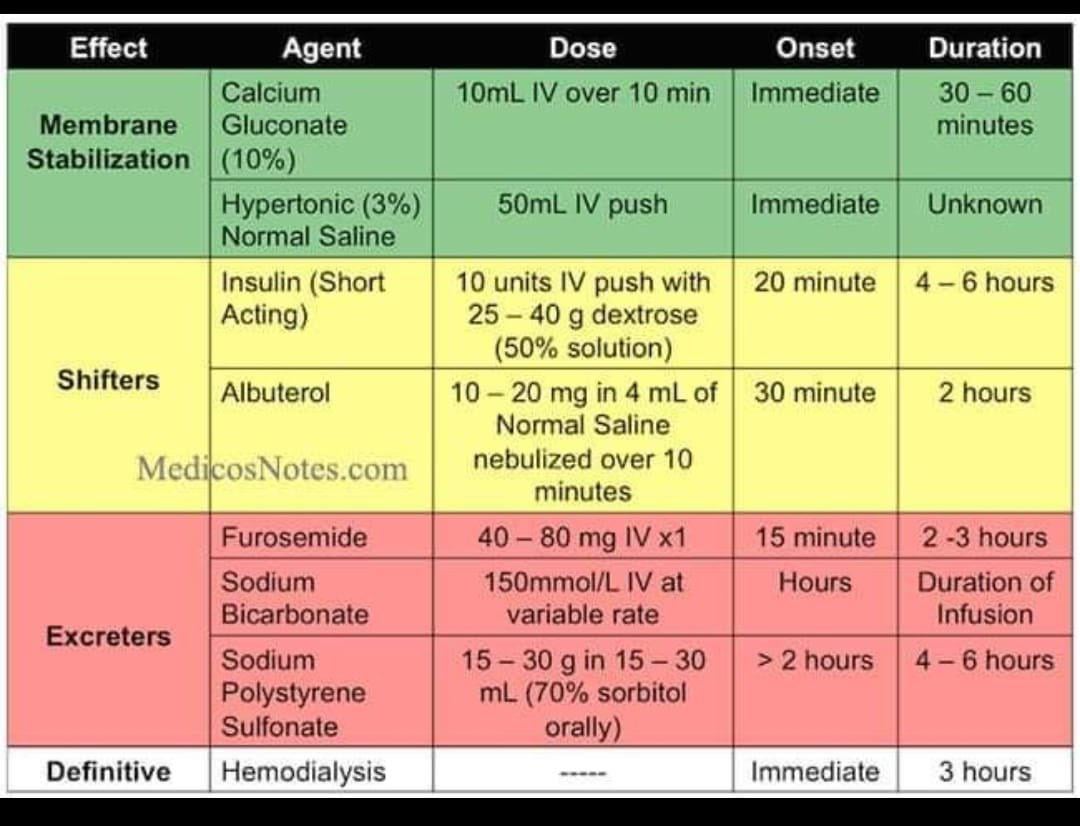
The main treatment for all types of renal tubular acidosis (RTA) is oral alkali therapy, typically with sodium bicarbonate or potassium citrate, to neutralize excess acid in the blood and restore normal pH balance.
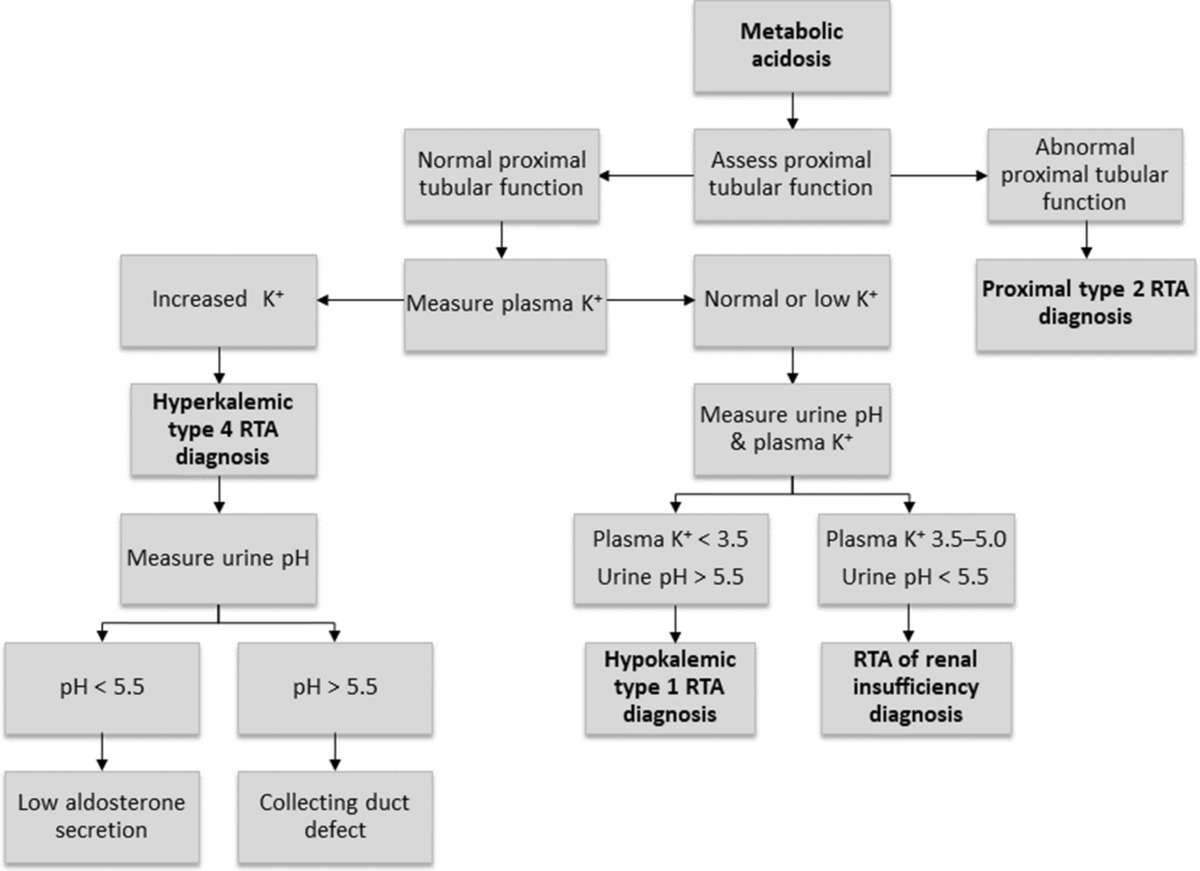
How does treatment differ among the types of RTA?
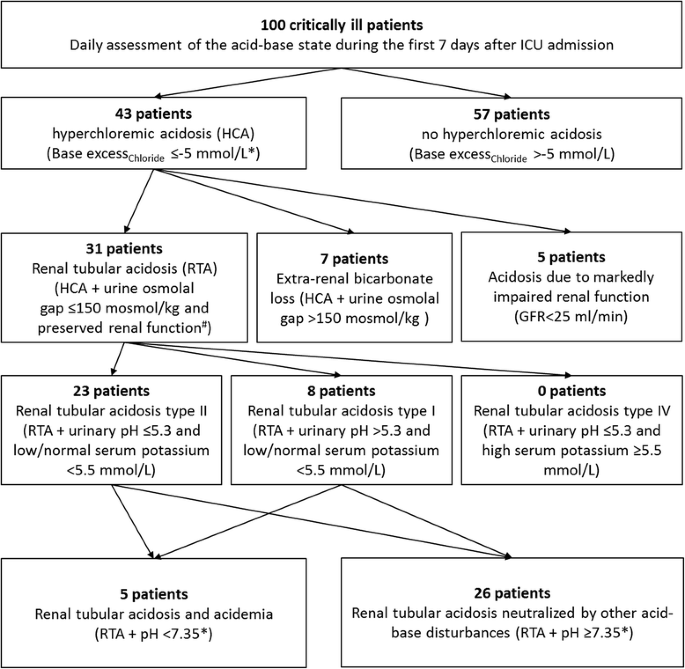
Type 1 (distal) and type 2 (proximal) RTA are treated with alkali therapy tailored by severity, with higher doses needed in proximal RTA. Type 4 (hyperkalemic) RTA treatment focuses first on addressing the underlying cause and cautiously using alkali if needed, while avoiding excess potassium.
Why is potassium citrate used in some cases of RTA?
Potassium citrate is preferred when patients have low potassium levels, as it both raises bicarbonate and replenishes potassium, especially important in type 1 RTA where hypokalemia is common.
What lifestyle or dietary changes support RTA treatment?
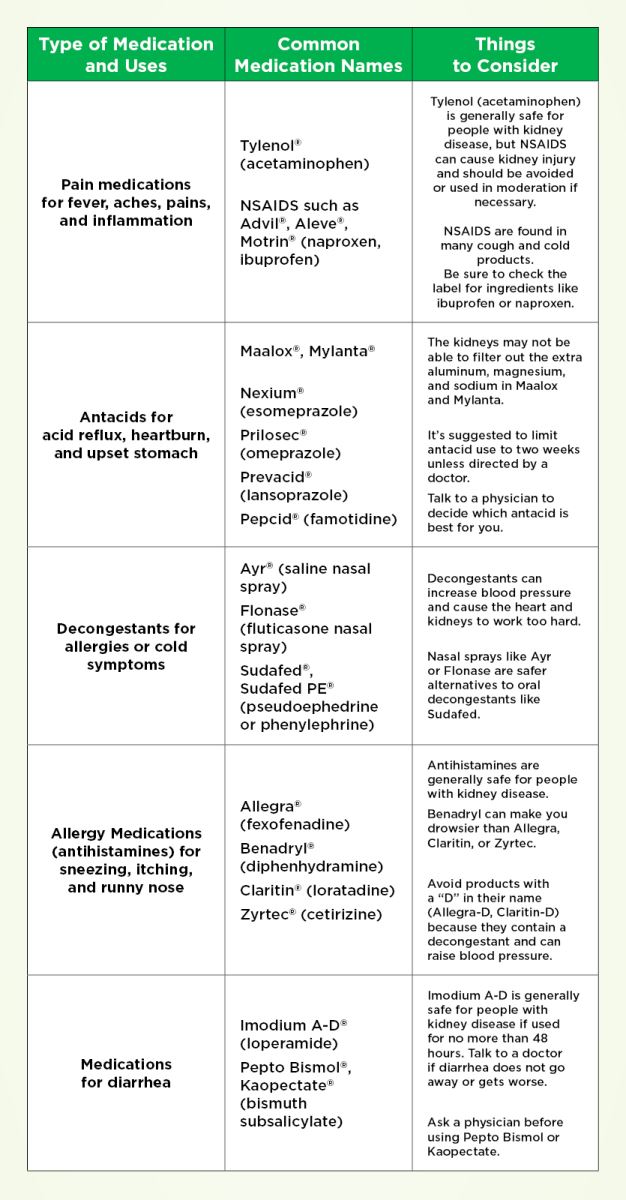
A diet rich in alkali-producing fruits and vegetables helps neutralize acid, while reducing intake of acid-producing animal proteins and processed high-phosphate foods supports treatment and bone health.
How often should patients with RTA be monitored during treatment?
Monitoring typically includes baseline labs before treatment, follow-up at 1 week, 1 month, and then every 3 to 6 months, focusing on bicarbonate levels, potassium, urine pH, and signs of complications like kidney stones or hypertension.