Staging Overview
What is Cancer Staging and Why It Matters
Staging is essentially the cancers report card. It tells doctors how big the tumor is, whether its spread to nearby lymph nodes, and if its traveled to distant parts of the body. This single snapshot guides everything from surgery choices to the need for chemo or radiation. In other words, knowing the stage helps you and your medical team map out the most effective, personalized plan.
The TNM System (8th Edition)
The TNM system breaks down cancer into three components:
T Tumor
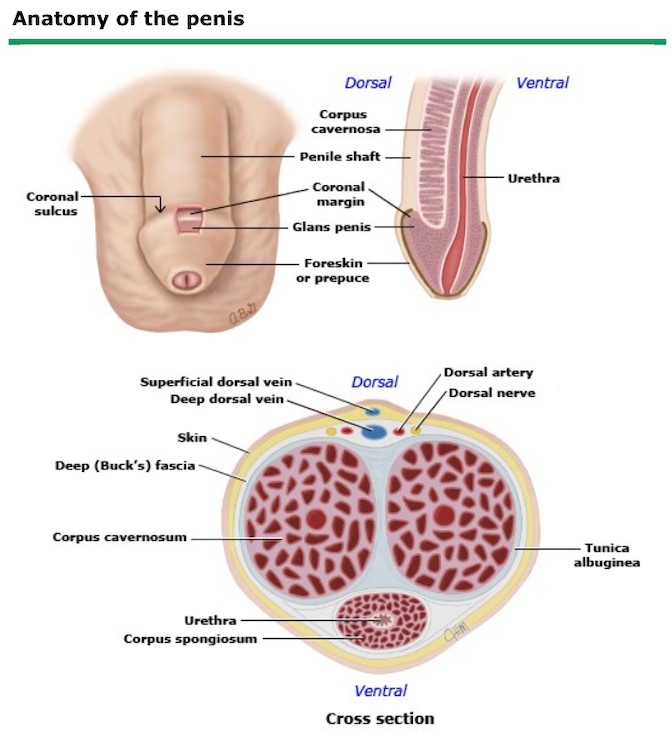
How deep the tumor has grown and whether its reached the corpora cavernosa (the erectile tissue) or the urethra. Sizes are measured in centimeters and depth of invasion.
N Nodes
Whether cancer has settled in the inguinal (groin) lymph nodes, or moved further up to the pelvic nodes. Fixed or matted nodes usually signal a more advanced stage.
M Metastasis
Any distant spreadlike to the lungs, liver, or bones. This moves the cancer straight to stageIV.
When you combine these letters into a code (for example, T2N1M0), the American Joint Committee on Cancer (AJCC) translates it into a stage from 0 to IV that most patients recognize.
AJCC Stage Grouping (0IV)
Heres the quick conversion:
- Stage0 Carcinoma in situ (confined to the surface)
- StageI Small tumor, no node involvement
- StageII Larger or deeper tumor, still no nodes
- StageIII Any tumor with positive regional nodes
- StageIV Distant metastasis
Understanding this ladder lets you ask the right questions at your appointments: Whats my T, N, M?, What does that mean for my treatment?, Whats the outlook?
StagebyStage Details
Stage0 (Carcinoma in Situ)
This is the earliest catchabnormal cells stuck on the skins surface, not yet invading deeper layers. You might notice a flat, red patch or a small ulcer that refuses to heal. Because its confined, surgery (often a simple excision) can be curative. Survival rates are excellentover 95% fiveyear survival according to the .
Stage1 (Stage1 Penile Cancer Survival Rate)
At this point the tumor is 2cm and stays within the inner layers of the penis. Symptoms can still be mildperhaps a painless ulcer or a slightly raised area. Surgery can range from a conservative local excision to a partial penectomy if needed. The good news? The fiveyear survival hovers around 8085%.
Stage2
The cancer has breached into deeper tissueusually the corpora cavernosa or spongiosumbut lymph nodes are still clear. You might feel more discomfort, a noticeable lump, or changes in urinary flow. Treatment often involves a partial penectomy, sometimes combined with sentinelnode biopsy to doublecheck the nodes. Fiveyear survival dips slightly to about 7080%.
Stage3 (Stage3 Penile Cancer Life Expectancy)
Now the regional lymph nodes are involvedeither fixed inguinal nodes or spread to the pelvic area. Symptoms can include swelling, pain, or even a foulsmelling discharge. Because the cancer is moving beyond the primary site, doctors usually add chemotherapy or radiation to surgery. Life expectancy varies, but median survival is roughly 23years, and fewer than 30% of patients reach five years.
Stage4 (Stage4 Penile Cancer Symptoms & Life Expectancy)
This is the most serious level: cancer has traveled to distant organs (lungs, liver, bones). You may notice weight loss, persistent pain, new skin lesions, or bone aches. Treatment shifts toward palliative intentmeaning the goal is to control symptoms and prolong quality of life. Median survival sits around 1218months, though some newer targetedtherapy trials show promise.
RealWorld Snapshot
Imagine Tom, a 58yearold who ignored a small ulcer for months. When he finally saw his urologist, a biopsy revealed StageIII disease with positive pelvic nodes. After a partial penectomy, he underwent combination chemoradiation. Six months later, his scans showed stable disease, and hes now back to gardeningthough hes on close surveillance. Stories like Toms illustrate how early detection dramatically shifts outcomes.
Treatment Guidance
Surgery Options by Stage
Heres a quick rundown:
- Stage0I: Local excision, laser ablation, or circumcision.
- StageII: Partial penectomy (removing part of the shaft) to achieve clear margins.
- StageIIIIV: Total penectomy may be necessary, often coupled with node dissection.
Radiation & Chemotherapy
Radiation can be used as the primary curative modality for patients who cant undergo surgery, especially in early stages. In later stages, its combined with chemotherapy (usually a platinumbased regimen) to shrink nodal disease.
Targeted & Immunotherapy
Clinical trials are exploring agents like pembrolizumab for metastatic (StageIV) penile cancer. While still investigational, early data suggest a modest improvement in progressionfree survival for a subset of patients. , these options may become standard in the next few years.
Treatment Decision Flowchart
| Stage | Primary Treatment | Adjunct Therapy | Typical Survival |
|---|---|---|---|
| 0I | Local excision / laser | None (occasionally radiation) | 8095% 5yr |
| II | Partial penectomy | Sentinelnode biopsy | 7080% 5yr |
| III | Partial/total penectomy + node dissection | Chemo + radiation | ~30% 5yr |
| IV | Palliative surgery (if needed) | Chemo, radiation, clinical trials | 1218mo median |
Radiology Imaging
Standard Scans for Staging
Accurate staging leans heavily on imaging:
- MRI of the penis: Gives detailed softtissue resolution to gauge depth (critical for Tcategory).
- CT of chest/abdomen/pelvis: Looks for nodal involvement and distant spread.
- PETCT: Particularly useful in StageIIIIV to spot hidden metastases.
- Ultrasound with Doppler: Helpful for evaluating inguinal lymph nodes when CT is equivocal.
Radiology Checklist for Patients
Before your scan, consider asking your doctor these questions:
- Will the MRI use a contrast agent?
- Do I need a bowel prep before a pelvic CT?
- How will the results affect my treatment plan?
- Is a PETCT recommended based on my stage?
Sample Radiology Report Snippet
"MRI demonstrates a 2.3cm T2 lesion invading the superficial corpus spongiosum without involvement of the corpora cavernosa. No evidence of extranodal extension. Bilateral inguinal nodes measure <1cm, appearing benign. No distant metastasis on CT chest/abdomen/pelvis."
Patient Stories
Johns EarlyStage Journey
John, 42, thought a lingering sore was just a minor irritation from cycling. After three weeks of nothing changing, his partner urged a doctor visit. A biopsy showed StageI disease, <2cm, no node involvement. He underwent a laser ablation and is now cancerfree after two years. His biggest takeaway? Dont dismiss persistent changeslisten to your body.
Marias Fight Through StageIII
Maria, 61, was diagnosed after her primary care physician noticed an enlarged inguinal node during a routine exam. Imaging revealed a 3cm primary tumor and N2 nodal disease (StageIII). She opted for a partial penectomy, followed by platinumbased chemo and localized radiation. Six months posttreatment, her scans show no active disease. Maria says, The team gave me hope, and the support groups kept me grounded.
Learning From Their Stories
Both John and Maria highlight two essential points:
- Early detection dramatically improves outcomes.
- A multidisciplinary teamurologist, medical oncologist, radiation oncologist, and supportive care servicesmakes a world of difference.
Further Reading & Trusted Sources
When youre digging deeper, rely on organizations that specialize in cancer care: for staging details and clinical guidance, review the TNM 8th edition resources linked in trusted references. For questions about prognosis like prostate cancer outlook or similar survival topics, your oncology team can help interpret how staging affects expected outcomes.
Conclusion
Understanding penilecancer stages is the first step toward taking control of your health. From the tiny, treatable lesions of Stage0 to the more complex challenges of StageIV, each level tells a clear story about how far the disease has traveled and what options lie ahead. Early detection, accurate imaging, and a collaborative treatment team can swing the odds in your favoroften dramatically. If you notice any persistent changes, schedule a checkup. And remember, youre not walking this path alone; credible resources, support groups, and compassionate clinicians are ready to help.
Whats your experience with cancer staging, or what question still lingers in your mind? Feel free to share belowyour story might be the encouragement someone else needs today.
FAQs
What are the different stages of penile cancer?
Penile cancer is grouped into stages 0‑IV based on tumor size, depth of invasion, lymph‑node involvement, and distant spread. Stage 0 is carcinoma in situ; Stage I‑II are localized tumors; Stage III involves regional lymph nodes; Stage IV indicates distant metastasis.
How does the TNM system determine the stage?
The TNM system assigns a code: T (size and depth of the primary tumor), N (presence and extent of regional lymph‑node involvement), and M (distant metastasis). These codes are then converted by the AJCC into the overall stage group (0‑IV).
What treatment options are typical for early‑stage penile cancer?
For Stage 0‑I disease, doctors often use local excision, laser therapy, or circumcision. These procedures aim to remove the tumor while preserving as much penile tissue as possible.
When is chemotherapy or radiation recommended?
Chemotherapy and/or radiation are usually added for Stage III disease (regional node involvement) and Stage IV (distant spread) to shrink tumors, control nodal disease, and improve survival chances.
What is the outlook for each stage?
Five‑year survival rates are >95 % for Stage 0, about 80‑85 % for Stage I, 70‑80 % for Stage II, roughly 30 % for Stage III, and median survival of 12‑18 months for Stage IV, although newer targeted therapies are improving outcomes.