Below, Ill walk you through the options, what you can realistically expect, and how to make the choices that feel right for you. Think of this as a friendly chat over coffeeno dry textbook jargon, just honest, helpful info.
Quick Answers
Lets start with the burning questions most people have when they first hear metastatic sarcoma.
What are the main goals of metastatic sarcoma treatment?
Were not talking about a miracle cure (more on that later). Instead, the goals are threefold: control the disease, relieve symptoms, and extend qualityoflife years. Think of it like steering a car on a winding roadyou may not get straight to the destination quickly, but you can keep the ride smooth and safe.
Can metastatic sarcoma be cured completely?
Unfortunately, a complete cure is rare once the cancer has spread. However, longterm remission isnt impossible, especially when the disease responds well to treatment and the patient remains in good health. Its a nuanced answer, and your doctor can give you a personalized outlook based on tumor type, grade, and response to therapy.
What are the standard firstline drugs?
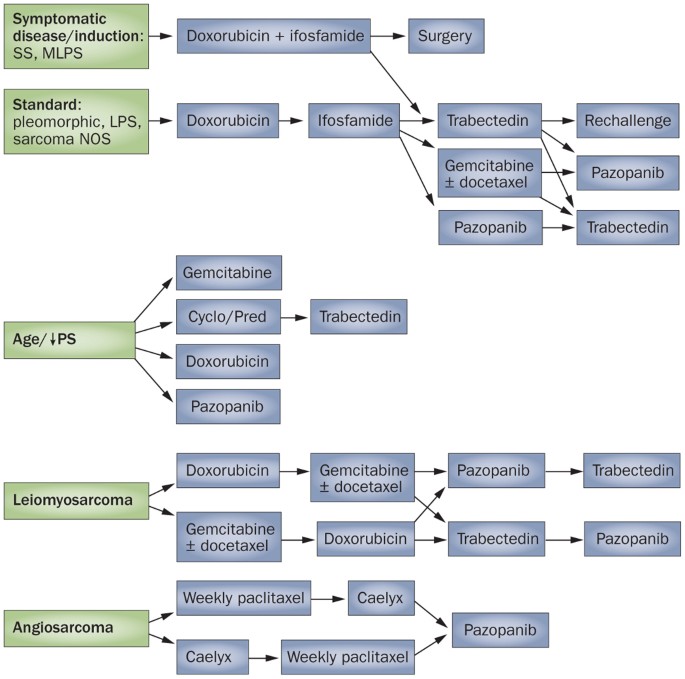
The backbone of systemic therapy usually starts with doxorubicinan anthracycline chemo thats been the gold standard for decades. Its often paired with ifosfamide to boost response rates. Below is a quick snapshot of the most common agents and what they bring to the table.
| Drug | Typical Dose | Response Rate | Key SideEffects |
|---|---|---|---|
| Doxorubicin | 75 mg/m IV (once every 3 weeks) | 2030% | Cardiotoxicity, nausea, alopecia |
| Ifosfamide | 910 g/m IV (over 35 days) | 1525% | Kidney strain, neurotoxicity, hemorrhagic cystitis |
| Pazopanib (targeted) | 800 mg oral daily | 1215% | Hypertension, liver enzyme rise, diarrhea |
| Gemcitabine+Docetaxel | Gemcitabine 900mg/m + Docetaxel 75mg/m IV (day 1, day 8, every 3 weeks) | 2030% | Myelosuppression, fatigue, skin rash |
How does treatment differ for stage4 versus highgrade sarcoma?
Both stage4 and highgrade sarcomas are aggressive, but the terminology matters. Stage4 indicates that the cancer has already spread to distant sites, while highgrade describes how quickly the tumor cells are dividing. In practice, highgrade tumors often get the same systemic regimen as stage4 disease because the risk of spreading is high.
What are the typical lifeexpectancy numbers?
Life expectancy varies widelyanywhere from 12months to several yearsdepending on factors like age, overall health, number of metastases, and how well the tumor responds to therapy. According to a study from the , patients with limited lung metastases who undergo aggressive treatment can sometimes live beyond five years.
Systemic Options
When you think systemic, imagine a flood of medicine traveling through every vein, hunting down cancer cells wherever they hide.
Chemotherapy: The backbone
Doxorubicin remains the first line because it attacks DNA replicationa hallmark of fastgrowing sarcoma cells. Its often given as a single agent, but adding ifosfamide can improve tumor shrinkage by 1015% in many cases. The tradeoff? More sideeffects, especially kidney irritation and a potential impact on heart health.
When the classic combo isnt suitableperhaps due to preexisting heart issuesdoctors might turn to gemcitabine plus docetaxel. This duo works well for many softtissue sarcomas and tends to have a slightly gentler sideeffect profile.
Targeted & Immunotherapy
Targeted agents like pazopanib lock onto specific molecular pathways that tumors use to grow. Theyre oral, which some patients find more convenient than IV chemo, but theyre not a magic bullet; response rates hover around 1015%.
Immunotherapy is an exciting frontier. Early trials with checkpoint inhibitors such as nivolumab and pembrolizumab have shown promise in a subset of sarcomas that express certain immunerelated markers. While not yet firstline, these drugs can be gamechangers for patients whose cancers are refractory to chemo.
ClinicalTrial Access
Because metastatic sarcoma is rare, many breakthroughs happen inside clinical trials. prostate removal life expectancy is an example of related survivorship content patients search for while exploring longterm outcomes; use trial registries to find studies based on your tumor type, location, and previous treatments. Joining a trial can offer access to cuttingedge therapies that arent otherwise available.
Managing SideEffects
Sideeffects can feel like a second battle, but with the right plan theyre manageable:
- Cardiotoxicity (doxorubicin): Baseline and periodic heartecho tests keep an eye on function.
- Kidney strain (ifosfamide): Hydration protocols and protective agents like mesna are standard.
- Myelosuppression (most chemo): Growthfactor injections (GCSF) and careful bloodcount monitoring help avoid infections.
- GI upset (pazopanib, gemcitabine): Antinausea meds, dietary tweaks, and staying hydrated make a big difference.
Balancing Benefits & Risks
Choosing a regimen isnt just about which drug works best?its also about what matters most to you. Some patients prioritize lengthening life as much as possible, even if it means tougher sideeffects. Others value a lighter treatment burden to stay active with family and hobbies. A solid decisionmaking framework looks like this:
- Discuss realistic response expectations with your oncologist.
- Identify personal priorities (e.g., time with grandchildren, travel, work).
- Weigh each drugs benefits against its sideeffect profile.
- Reevaluate regularly as your disease and life circumstances evolve.
Local Strategies
Even when the cancer has spread, local treatments can still play a crucial roleespecially if only a few lesions are causing trouble.
Surgical Resection of Isolated Metastases
When metastases are limited (often called oligometastatic), removing them surgically can improve both survival and quality of life. Candidates usually have good performance status, limited organ involvement, and tumors that are technically resectable. A retrospective analysis in Annals of Surgical Oncology found that patients who had lung metastasectomy lived a median of 34 years longer than those who didnt.
Stereotactic Body Radiotherapy (SBRT)
SBRT delivers very high doses of radiation in a few precise sessions. Its perfect for small lung or bone lesions that are hard to reach surgically. Success rates for local control exceed 80% in many series, and sideeffects are typically mild (fatigue, skin redness). Its also a good bridge to systemic therapy, shrinking tumors enough to make chemo more effective.
Thermal Ablation (Radiofrequency or Cryo)
Think of it as zapping the tumor with heat or freezing it solid. These techniques work best for lesions under 3cm and are often used for liver or kidney mets. Though data are limited, early reports suggest comparable control rates to surgery for carefully selected patients.
When to Combine Local + Systemic
One common pathway looks like: neoadjuvant chemo surgical resection adjuvant systemic therapy. This sequence can shrink tumors enough to make surgery safer and then mop up any microscopic disease left behind.
RealWorld Snapshot
Imagine a 52yearold teacher named Maya. She had three lung mets after her primary thigh sarcoma was removed. Her team gave her two cycles of doxorubicin/ifosfamide, which shrank two nodules dramatically. The third nodule, however, stayed stubborn. They opted for SBRT on that lesion, and within months her scans showed no active disease. Maya now continues on a lowdose pazopanib to keep any hidden cells in check, and shes back teaching art classessomething she feared shed have to give up.
Emotional & Practical Reality
Lets be realtalking about treatment is only half the story. Dealing with metastatic sarcoma also means navigating symptoms, lifeplanning, and emotional ups and downs.
Understanding Metastatic Sarcoma Symptoms
Symptoms depend on where the cancer has traveled. Common endstage sarcoma symptoms include:
- Persistent, deepseated pain (especially in bones or joints).
- Unexplained weight loss and fatigue.
- Shortness of breath or coughing if lungs are involved.
- Neurological signs (numbness, weakness) when the spine is affected.
Having a clear symptom checklist helps you and your healthcare team spot changes early and adjust treatment accordingly.
Life Expectancy: Numbers vs. Person
Statistical lifeexpectancy ranges can feel coldlike a number on a wall. But every persons story is unique. Factors that can nudge the needle upward include:
- Younger age at diagnosis.
- Fewer metastatic sites.
- Good response to firstline chemo.
- Access to clinical trials.
While we cant predict exact timelines, focusing on quality of the time you have often leads to better overall satisfaction.
Palliative Care & Support Services
Palliative care isnt just for the final weeks. Its an interdisciplinary approach that aims to control pain, manage sideeffects, and provide emotional support from day one. Think of it as a safety net that lets you stay in the drivers seat of your life, even when the road gets bumpy.
Financial & Insurance Navigation
Highcost drugs like doxorubicin and newer targeted agents can strain wallets. Here are a few tips:
- Ask your oncologists office for a financial counselormost cancer centers have them.
- Check whether your insurer requires prior authorization for specific chemo agents.
- Explore patientassistance programs offered by pharmaceutical companies (many have secretsauce discounts).
RealWorld Voices
Including real stories makes the data feel human. For example, Tom, a 38yearold software engineer, shared that joining a sarcoma support group helped him cope with the can sarcoma be cured completely question. Hearing that others had periods of remission gave him hope, even when his oncologist said the disease was incurable.
Takeaways
Metastatic sarcoma treatment is a complex, everevolving field, but the core ideas are simple:
- Systemic therapy (chemo, targeted drugs, immunotherapy) is the foundation.
- Local treatments (surgery, SBRT, ablation) can add extra control when metastases are limited.
- Balancing benefits and risks is a personal decisiontalk openly with your care team about what matters most to you.
- Support mattersclinical trials, palliative care, financial counseling, and community groups are all part of the roadmap.
So, whats the next step for you? Maybe its asking your oncologist about a clinical trial, setting up a meeting with a palliativecare specialist, or simply sharing your thoughts in the comments below. Whatever you choose, remember youre not navigating this alonetheres a whole network of experts, patients, and friends ready to walk beside you.
FAQs
What are the main goals of metastatic sarcoma treatment?
The primary goals are to control tumor growth, relieve symptoms caused by the cancer, and extend the patient’s quality of life rather than to cure the disease completely.
Which drugs are commonly used as first-line treatment for metastatic sarcoma?
Doxorubicin is the standard first-line chemotherapy agent, often combined with ifosfamide to increase effectiveness. Other options include gemcitabine plus docetaxel and targeted therapies like pazopanib.
Can metastatic sarcoma be cured?
A complete cure for metastatic sarcoma is rare. However, some patients achieve long-term remission depending on tumor type, response to treatment, and overall health.
When is surgery considered for metastatic sarcoma?
Surgery may be an option for patients with limited (“oligometastatic”) metastases, especially in the lungs, to improve survival and quality of life when the tumors are resectable.
What role does immunotherapy play in treating metastatic sarcoma?
Immunotherapy, including checkpoint inhibitors, is an emerging option showing promise in certain sarcoma subtypes, particularly for patients who do not respond to conventional chemotherapy.