If youre staring at a stack of medical papers and wondering, What exactly is the ALL treatment protocol? youve come to the right place. In a nutshell, the ALL (acute lymphoblastic leukemia) treatment protocol is a carefully staged chemotherapy plan that also may include targeted drugs, CNS protection, and sometimes a stemcell transplant. Knowing each phase, the differences for kids versus adults, and the newest targeted options helps you weigh benefits against risks and choose the safest path.
ALL Protocol Overview
First things first: why do we even call it a protocol? Because every step from the first steroid dose to the final maintenance pill follows a proven schedule designed to wipe out leukemia cells while keeping the body as healthy as possible. The modernall treatment protocol is built on three pillars:
- Induction the heavyhit phase that aims for complete remission.
- Consolidation/Intensification cleans up hidden disease.
- Maintenance lowdose therapy that stops the cancer from coming back.
Guidelines from the National Cancer Institute (NCI) and the American Society of Hematology are the gold standard for these steps, and they are updated regularly to incorporate breakthroughs like and CART cells.
Who designs the protocol?
It isnt a lone scientist working in a lab. A multidisciplinary team hematologists, pharmacists, radiation oncologists, and often a dedicated clinicaltrial group (think CALGB, COG, or the EWING Study) tailors the all treatment protocol pdf to the patients age, genetic risk factors, and overall health. That collaborative approach ensures the plan is both evidencebased and personalized.
Realworld example
Meet Maya, a 7yearold diagnosed with Bcell ALL. Her pediatric oncologist pulled the latest PDF, adjusted the dosing for her weight, and added a CNS prophylaxis schedule. Within six weeks, Maya entered remission a testament to how a wellcrafted protocol can change lives.
Phase by Phase Details
Induction The Kickoff
This is the all induction protocol that most families hear about. The goal is to push the leukemia into complete remission (CR) meaning no cancer cells are detectable in the bone marrow. Typical drugs include:
- Vincristine
- Prednisone
- Lasparaginase
- Daunorubicin (often for adults)
For pediatric patients, the doses are weightbased; adults may receive slightly higher amounts but also a broader supportivecare package.
Induction drug list (pediatric vs. adult)
| Drug | Pediatric Dose | Adult Dose |
|---|---|---|
| Vincristine | 1.5mg/m (max 2mg) | 2mg/m (max 2mg) |
| Prednisone | 60mg/m daily | 1mg/kg daily |
| Lasparaginase | 10,000U/m IM | 6,000U/m IV |
| Daunorubicin | 30mg/m IV |
Consolidation / Intensification
Once remission is achieved, the next step attacks any hidden cells that survived induction. Highdose methotrexate, cytarabine, and cyclophosphamide are common, and many protocols now sprinkle in a tyrosinekinase inhibitor (TKI) for Philadelphiapositive (Ph) disease.
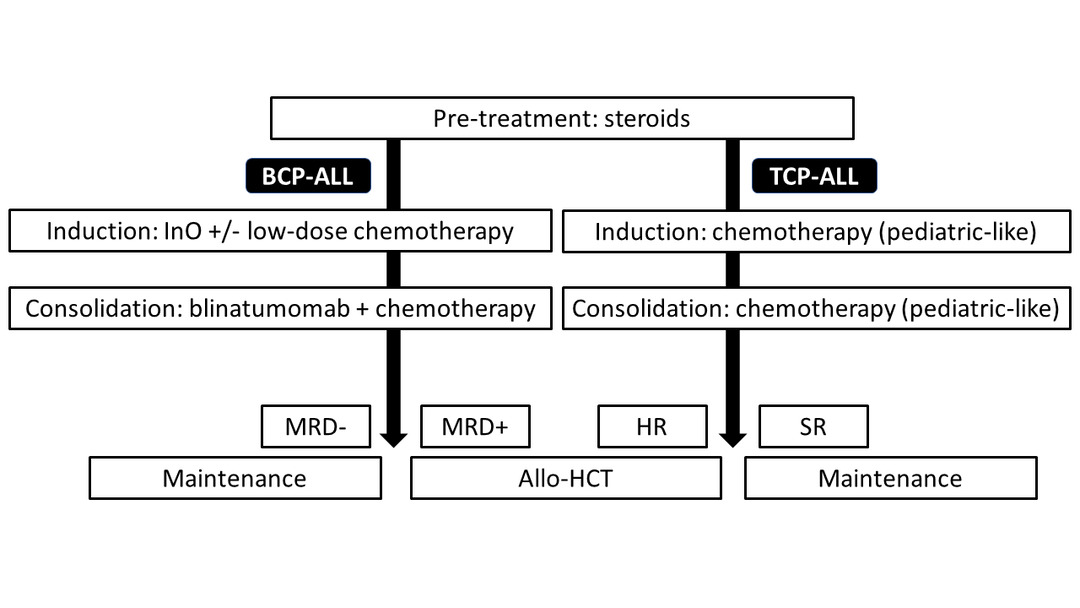
Bcell vs. Tcell comparison
| Aspect | Bcell ALL | Tcell ALL |
|---|---|---|
| Key Drug | Inotuzumab ozogamicin | Nelarabine |
| Targeted Agent | Blinatumomab (BiTE) | None yet, trials ongoing |
| Typical Toxicities | Hepatotoxicity | Neurotoxicity |
Maintenance The Long Haul
Maintenance is the all chemotherapy regimen that stretches over 23years (longer for children). Oral 6mercaptopurine (6MP) and weekly methotrexate keep the disease at bay while your body recovers from the heavier earlier phases.
Adherence checklist
- Set a daily alarm for 6MP.
- Keep a medication log (paper or app).
- Schedule monthly blood tests to monitor counts.
- Discuss dose adjustments with your oncologist if you notice side effects.
CNS Prophylaxis Guarding the Brain
Leukemia loves hiding in the central nervous system. Intrathecal methotrexate (injected directly into the spinal fluid) and, for highrisk patients, lowdose cranial radiation are nonnegotiable parts of any all treatment protocol. The benefits of preventing CNS relapse far outweigh the shortterm headaches and nausea.
Risks vs. Benefits infographic
Imagine a tiny shield protecting your brain the shields weight is the occasional nausea, but the protection is preventing a lifethreatening relapse. Thats the balance we aim for.
Specialized Treatment Options
Pediatric ALL Treatment Protocol
Kids arent just small adults. Pediatric protocols incorporate agespecific dosing and riskadapted therapy. The Children's Oncology Group (COG) releases a 2024 pediatric that many hospitals follow. It emphasizes reduced toxicity without compromising cure rates.
Downloadable PDF (example)
You can access the latest pediatric guidelines directly from the COG website just look for the Pediatric ALL Treatment Protocol (2024) PDF. Its a quick read (about 25pages) and includes dosing charts for every drug.
Adult ALL Treatment Protocol
Adults often tolerate chemotherapy differently and may have coexisting conditions. The acute lymphoblastic leukemia treatment protocol for adults therefore integrates TKIs for Ph cases (imatinib, dasatinib) and may consider early stemcell transplant for highrisk genetics.
Case vignette
John, a 45yearold with Ph ALL, started on imatinib plus standard induction chemo. By week4 his bonemarrow blast count dropped to 0%. After consolidation, he proceeded to an allogeneic transplant a path that aligns with current adult guidelines.
Relapsed ALL Treatment Protocol
When the disease comes back, the strategy shifts. Salvage chemotherapy, novel antibodies (blinatumomab, inotuzumab), and CART cell therapy become frontline options. The relapsed all treatment protocol often includes a bridge to transplant if the patient responds.
Decisiontree for relapse
1 Verify relapse with bonemarrow biopsy.
2 Assess eligibility for CART (age, prior therapies).
3 If CART isnt an option, start salvage chemo + targeted antibody.
4 Plan for transplant if remission achieved.
Finding Official PDFs
Searching all treatment protocol pdf can return a mix of reputable and outdated files. Heres a quick credibility checklist:
- Published by a recognized organization (NCI, ASH, COG).
- Last updated within the past 12months.
- Includes author credentials and peerreview notes.
- Provides clear dosing tables and references.
Official sources
Visit the NCIs , the American Society of Hematology (ASH) site, or the COG portal for the most trustworthy PDFs. Download them, print a cheatsheet, and keep it on your fridge its a lifesaver during busy chemo weeks.
Balancing Benefits and Risks
Common side effects
Every phase brings its own set of challenges:
- Myelosuppression low blood counts, leading to infections.
- Neuropathy tingling from vincristine.
- Mucositis sore mouth lining.
- Fatigue especially during maintenance.
Supportive care (GCSF, antinausea meds, oral rinses) can keep these in check. Ask your team about prophylactic antibiotics if you have a history of infections.
Longterm risks
While the cure rate for childhood ALL exceeds 90%, survivors sometimes face late effects:
- Secondary cancers (especially after cranial radiation).
- Cardiac toxicity from anthracyclines.
- Infertility a discussion that should happen before treatment begins.
Surveillance timeline
| Year(s) | Recommended Test |
|---|---|
| 02 | Complete blood count every 3months |
| 35 | Echocardiogram annually |
| 5+ | Screen for secondary malignancies per guidelines |
When to explore experimental options
If standard chemo isnt enough, clinical trials can offer access to the newest therapies. Platforms like let you filter by ALL and PhaseII/III. Talk to your oncologist they often have trial coordinators ready to help.
Patient Experience Stories
Story 1 A childs journey
Emma, a 5yearold, started treatment in September 2023. Her family kept a daily diary, noting every dose, side effect, and triumph. By week8, Emmas marrow was clear. The family says the diary made the nightmare feel manageable because it turned the protocol into a story they could follow together.
Key takeaway
Documenting the all treatment protocol doesnt just help doctors; it empowers families to see progress in real time.
Story 2 An adults relapse and recovery
Mark, 38, faced a relapse two years after his initial remission. He enrolled in a trial for blinatumomab, a bispecific Tcell engager, followed by a matchedsibling transplant. Today, Mark is three years posttransplant and volunteers at a local cancer support group, reminding new patients that relapse isnt the end, its a new chapter.
Key takeaway
Modern relapsed ALL treatment protocols combine immunotherapy with transplant possibilities, offering hope even after the disease returns.
Conclusion
Understanding the ALL treatment protocol from inductions heavyhit start to maintenances gentle, longterm watch equips you to ask the right questions, track progress, and collaborate with your care team. Whether youre scrolling through a all treatment protocol pdf for the first time or weighing a new targeted drug, remember that each step is built on decades of research and realworld experience. Download the official PDFs, keep a treatment diary, and dont hesitate to discuss clinicaltrial options if standard therapy feels insufficient.
Whats been your experience with an ALL protocol? Have you found a particular resource or tip that made a difference? Share your story in the comments were all in this together, and your insight could be exactly what someone else needs to hear.
FAQs
What are the three main phases of the ALL treatment protocol?
The protocol consists of induction (to achieve remission), consolidation/intensification (to eliminate hidden disease), and maintenance (low‑dose therapy to prevent relapse).
How does the ALL protocol differ between children and adults?
Pediatric protocols use weight‑based dosing and often reduce toxicity, while adult regimens may include higher drug doses, additional targeted agents, and more supportive‑care measures.
When is CNS prophylaxis required in ALL treatment?
CNS prophylaxis is a standard part of all ALL protocols, using intrathecal methotrexate and, for high‑risk patients, low‑dose cranial radiation to prevent leukemia spread to the brain and spinal fluid.
What targeted therapies are available for relapsed ALL?
Relapsed protocols may incorporate monoclonal antibodies such as blinatumomab or inotuzumab, tyrosine‑kinase inhibitors for Ph⁺ disease, and CAR‑T cell therapy when eligible.
How can patients stay adherent to the long‑term maintenance phase?
Tip: set daily alarms for oral 6‑mercaptopurine, keep a medication log, attend monthly labs, and discuss any side effects promptly with the oncology team.