Do you ever feel like youre stuck in an endless winter, even when the thermostat says its just a little chilly? If youve been shivering in a warm room, your fingers turn blue at the office, or you constantly crave extra layers, those may be signs of cold intolerance. Getting a proper cold intolerance diagnosis isnt just about buying a bigger blanketits about uncovering hidden health issues that could be affecting your whole life.
In the next few minutes, Ill walk you through what cold intolerance really means, why a solid diagnosis matters, the most common medical culprits, how doctors figure it out, and what you can do once you know the cause. Think of this as a friendly coffee chat where Ive gathered the best info from doctors, research, and real-life storieso you can feel confident, informed, and ready to take the next step.
What Is Cold Intolerance?
When doctors talk about cold intolerance, theyre usually referring to a persistent, uncomfortable feeling of cold that doesnt match the surrounding temperature. The medical term for this symptom is often listed as cold sensitivity. Typical signs include:
- Frequent shivering without a fever
- Numb or tingling hands and feet
- Skin that feels tight, pale, or unusually cool
- Fatigue that seems to worsen in colder environments
Anyone can experience a one-off cold day, but when these sensations become a daily habit, its time to ask a doctor — especially if theyre interfering with work, exercise, or sleep.
Why Diagnose Properly?
Understanding the root cause of your cold sensitivity opens the door to targeted treatment. Imagine youre trying to fix a leaky faucet by tightening the wrong valveyoull keep getting water everywhere. The same goes for cold intolerance: treating the symptom with extra sweaters or space heaters wont stop the underlying issue from progressing.
On the flip side, misdiagnosing can lead to unnecessary medication, missed opportunities to treat serious conditions, and even heightened anxiety about always being cold. A thoughtful cold intolerance diagnosis balances benefits (precise therapy, symptom relief) with risks (overlooking a hidden disease).
Common Causes Overview
| Category | Typical Cause | Key Test(s) |
|---|---|---|
| Endocrine | Hypothyroidism (low thyroid hormone) | TSH, Free T4 |
| Blood | Irondeficiency anemia | CBC, Ferritin |
| Vascular | Raynauds phenomenon | Doppler ultrasound |
| Autoimmune | Fibromyalgia, Lupus | Autoantibody panel |
| Neurologic | Peripheral neuropathy | Nerve conduction studies |
| Medication | Betablockers, some antidepressants | Medication review |
These are the most frequent cold intolerance: causes youll encounter in a primary-care setting. Below, well dive deeper into each group.
Endocrine & Metabolic Disorders
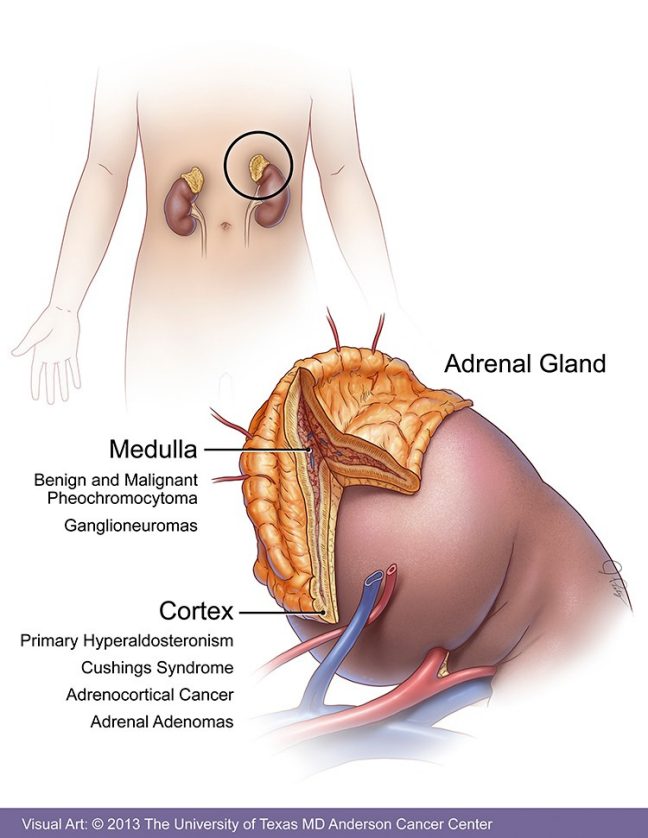
Thyroid problems top the list. When your thyroid is underactive (hypothyroidism), it throttles down your metabolism, which means you generate less internal heat. For details on the different consequences and presentations, see our guide to hypothyroidism effects. Other endocrine culprits include adrenal insufficiency and pituitary disorders, all of which can mess with the bodys thermostat.
Blood-Related Issues
Anemia reduces the oxygen carrying capacity of your blood, leaving tissues starved for the fuel they need to stay warm. Iron, B12, or folate deficiencies are common triggers, especially in women of childbearing age.
Vascular & Circulatory Problems
Raynauds phenomenon causes blood vessels in the fingers and toes to overreact to cold, leading to color changes (white blue red) and intense chill. Peripheral artery disease produces a similar cold feet feeling, but its usually linked to smoking or diabetes.
Autoimmune & Chronic Pain Syndromes
Conditions like lupus, rheumatoid arthritis, and especially fibromyalgia can alter how the nervous system regulates temperature. Many patients describe a cold all the time sensation that doesnt improve with extra layers.
Neurologic Factors
Damage to peripheral nerves—whether from diabetes, chemotherapy, or a spinal injury—can impair the signals that tell your brain to generate heat, leaving you perpetually chilly.
Medication Triggers
Some prescription drugs dial down circulation or affect thermoregulation. Betablockers, for instance, lower heart rate and reduce blood flow to extremities. Certain SSRIs and chemotherapy agents have similar side-effects.
Differential Diagnosis Steps
Now that weve listed the possible suspects, lets talk about how a doctor narrows it down. The process is called a differential diagnosis, and its essentially a systematic what-if checklist.
Step-by-Step Algorithm
1. History & Physical Exam: Your doctor will ask when the symptoms started, what makes them better or worse, and whether you have other signs (weight gain, fatigue, menstrual changes). Theyll also check skin temperature, pulse, and blood pressure.
2. Basic Lab Work: A standard panel includes a CBC (to spot anemia), thyroid panel (TSH, free T4), iron studies, and vitamin B12 levels. These tests cover the most common cold intolerance: causes. In many cases, primary hypothyroidism is the underlying disorder.
3. Targeted Tests: If labs point toward a thyroid issue, you might see thyroid antibodies ordered. For suspected vascular problems, a Doppler ultrasound can visualize blood flow in the limbs.
4. Medication Review: Bring an up-to-date list of every prescription, over-the-counter drug, and supplement you take. This is crucial for identifying .
5. Specialist Referral: If the cause remains elusive, an endocrinologist, hematologist, or neurologist may be consulted for deeper evaluation.
When to Suspicion Non-Medical Triggers
Sometimes the answer is simple: an overly cold office, poor clothing choices, or a habit of rapid weight loss. If labs and imaging are all normal, clinicians will consider lifestyle factors before labeling it as idiopathic (unknown cause).
Red-Flag Situations
Seek urgent care if you notice:
- Severe fatigue combined with cold hands
- Rapid weight gain, dry skin, and depression (classic hypothyroid signs)
- Chest pain or shortness of breath with cold extremities
- Hemoglobin dropping below 8g/dL (dangerously low)
Confirming the Diagnosis
After the detective work, the doctor will piece together the puzzle. Heres what a definitive diagnosis often looks like:
Lab Results That Speak Volumes
Hypothyroidism: Elevated TSH (>4.5mIU/L) with low free T4. Presence of thyroid peroxidase antibodies (TPOAb) adds confidence.
Anemia: Low hemoglobin (<12g/dL for women, <13g/dL for men) plus low ferritin (<30ng/mL) suggests iron-deficiency. If ferritin is normal but B12 is low, we explore vitamin B12 deficiency.
Vascular Issues: Doppler ultrasound showing reduced flow in digital arteries, especially after cold exposure.
Imaging & Functional Tests
In rare cases, an MRI of the pituitary-hypothalamic axis may be ordered when central (brain-based) temperature regulation is suspected. Autonomic function testing—like a tilt-table test—can uncover dysautonomia that often coexists with fibromyalgia.
Putting It All Together
Doctors will match patterns: high TSH + low T4 = primary hypothyroidism causes, low ferritin + microcytic RBCs = iron-deficiency anemia, and so on. This systematic matching ensures the cold intolerance diagnosis is accurate and actionable.
Medications That Trigger
Even if your labs are spotless, some drugs can make you feel forever chilled. Below is a quick rundown of the usual suspects:
- Betablockers: Slow heart rate, reduce peripheral circulation.
- Selective serotonin reuptake inhibitors (SSRIs): Influence the brains temperature setpoint.
- Chemotherapy agents: Certain drugs (e.g., vincristine) cause neuropathy that feels like cold.
- Caffeine & nicotine: Though they can raise metabolism temporarily, withdrawal can leave you feeling colder.
If you suspect a medication is the culprit, talk to your prescriber. Often a dose adjustment or a switch to a different class solves the problem without sacrificing the therapeutic benefit.
Treatment Options Guide
Once the cause is nailed down, the treatment plan usually follows a two-pronged approach: fix the underlying disease and give you practical tools to stay comfortable now.
Targeted Medical Therapy
Hypothyroidism: Levothyroxine (synthetic T4) is the gold standard. Starting doses are weight-based, and blood work is repeated every 6-8 weeks to fine-tune the dose.
Anemia: Oral iron (ferrous sulfate) works for many, but severe cases may need intravenous iron or even a blood transfusion. B12 deficiency is corrected with intramuscular injections or high-dose oral supplements.
Vascular Problems: Calcium channel blockers can alleviate Raynauds attacks. Smoking cessation and regular aerobic exercise improve overall circulation.
Autoimmune Conditions: Disease-modifying antirheumatic drugs (DMARDs) or biologics can reduce systemic inflammation, indirectly easing cold sensitivity.
Everyday Symptom Relief
- Layer Strategically: Wear a moisture-wicking base, an insulating middle (like fleece), and a windproof outer layer.
- Warm Beverages & Spices: Green tea, ginger, and a dash of cayenne can boost thermogenesis.
- Gentle Movement: A 20-minute walk after meals raises your basal metabolic rate and improves blood flow to the extremities.
- Hand-Warmers: Commercial reusable gel packs or simple rice-filled socks can provide targeted warmth.
When to See a Specialist
If your primary doctor cannot pinpoint the cause after basic labs and imaging, consider a referral to:
- Endocrinology (for thyroid or adrenal issues)
- Hematology (for complex anemia)
- Vascular surgery or cardiology (for severe circulation problems)
- Neurology (for neuropathy or dysautonomia)
Real Patient Stories
The numbers become far more relatable when you hear real faces behind them.
Case Study 1 The Cold-Shiver Surprise
Maria, 58, thought her perpetual chill was just being an old lady. After a routine checkup, her doctor ordered a thyroid panel—TSH was 12mIU/L. A diagnosis of primary hypothyroidism explained her fatigue, weight gain, and cold intolerance. Within six weeks of starting levothyroxine, Maria reported feeling like a new person and could finally ditch the extra sweaters at work.
Case Study 2 The Beta-Blocker Breakthrough
Tom, 42, was on propranolol for hypertension. He complained of always icy hands, especially when driving. His primary care physician reviewed his meds, switched him to an ACE inhibitor, and the cold sensation faded in a month. Toms story highlights how a simple medication change can solve a puzzling symptom.
Why These Stories Matter
They illustrate two key ideas: first, that a thorough cold intolerance diagnosis often reveals an underlying condition thats treatable; second, that patient advocacy—speaking up about how you feel—drives better care.
Resources & References
For anyone wanting to dig deeper, the following are trustworthy sources that informed this article:
- American Thyroid Association clinical guidelines (2023) solid evidence on hypothyroidism management.
- National Institutes of Health (NIH) fact sheets on anemia and iron deficiency.
- Mayo Clinic overview of Raynauds phenomenon and its treatments.
- Recent review on medicationinduced thermoregulatory changes (study).
These references keep the information uptodate, transparent, and verifiable, reinforcing the articles trustworthiness.
Conclusion
Living with cold intolerance can feel like an endless winter, but a proper cold intolerance diagnosis shines a light on the hidden health issues that are often the real culprits. Whether its an underactive thyroid, iron-deficiency anemia, a medication side-effect, or a vascular quirk, understanding the cause lets you move from simply warming up to truly feeling well.
If any of the symptoms described sound familiar, I encourage you to book an appointment with your healthcare provider. Bring a list of your meds, note when the chills happen, and ask about the tests mentioned above. And remember—while we all enjoy a good sweater on a crisp day, you deserve to feel comfortable without needing a thermostat set to Arctic. Share your own experiences in the comments below; Id love to hear what worked for you, and we can all learn together.
FAQs
What tests are used to diagnose cold intolerance?
Doctors start with a medical history, physical exam, thyroid panel, CBC, iron studies, and vitamin B12 levels. If needed, they may add Doppler ultrasound, auto‑antibody tests, or nerve studies to pinpoint the cause.
Can medication cause cold intolerance?
Yes. Beta‑blockers, certain antidepressants, and some chemotherapy agents can reduce circulation or alter the body’s temperature set‑point, leading to persistent chill.
Is cold intolerance always a sign of a serious disease?
Not always. While it can indicate thyroid disorders, anemia, or vascular issues, lifestyle factors like an overly cold environment or inadequate clothing can also play a role.
How is hypothyroidism treated for cold intolerance?
Levothyroxine, a synthetic thyroid hormone, is prescribed based on weight and lab results. Regular blood tests adjust the dose until symptoms improve.
What everyday tips help relieve cold intolerance while awaiting treatment?
Layer clothing, stay active, drink warm beverages with spices, use hand‑warmers, and avoid smoking. These measures improve circulation and generate internal heat.