Finding a lump in your neck can feel like stumbling onto a surprise party you never asked for. The short answer? Most thyroid lumps are harmless, but a few can hide trouble that needs attention. Below you'll get the facts you're looking for what to watch for, when to call a doctor, and how to move forward with confidence.
Understanding Thyroid Lump
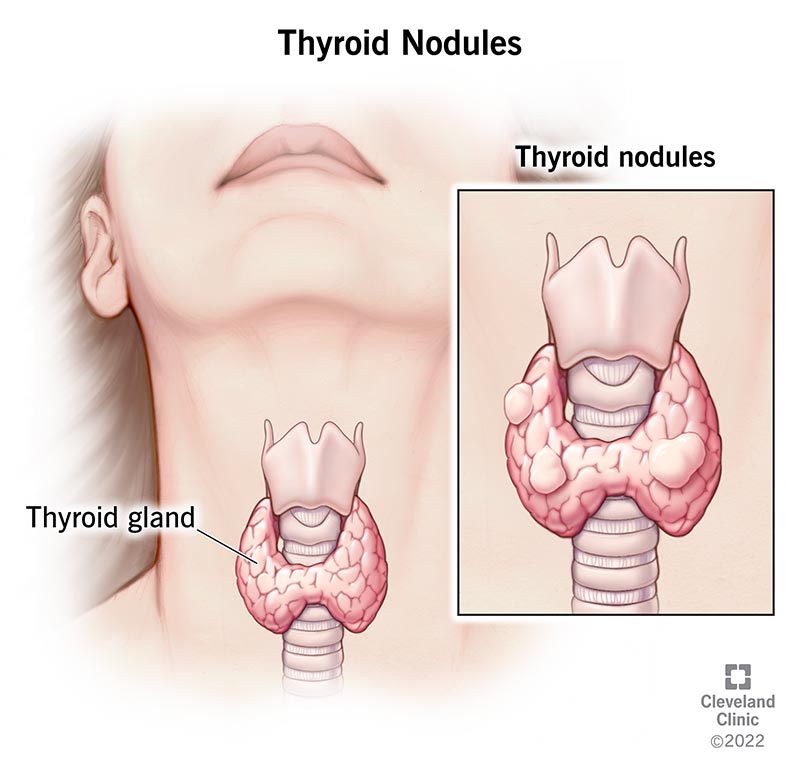
What exactly is a thyroid lump?
The thyroid is a butterfly-shaped gland sitting just below your Adam's apple. A lump can be a solid nodule (a cluster of cells) or a fluid-filled cyst. Both show up as a bump on ultrasound, but they behave very differently.
How common are they?
Studies suggest that up to 65% of adults will have at least one thyroid nodule by age 60most of them never cause a problem. Women are more likely to notice them, thanks to hormonal shifts that make the gland a bit more talkative.
Solid vs. cystic: why it matters
Solid nodules can be benign or, in rare cases, cancerous. Cysts are usually filled with clear fluid and tend to stay benign, though they can cause discomfort if they grow large.
Quick snapshot
| Type | Typical Size | Usual Risk |
|---|---|---|
| Solid nodule | 0.54cm | 46% malignant |
| Cyst | Variable | Usually benign |
Common Lump Symptoms
What you might actually feel
Most people first notice a painless bump in the front of their neck. You might also feel:
- A sensation of fullness or tightness when you swallow
- Occasional hoarseness (the recurrent laryngeal nerve runs nearby)
- Rarely, pain that radiates to the jaw or ear
Woman-specific clues
Hormonal fluctuations can make thyroid nodules behave a little differently in women. You may experience:
- Changes in menstrual regularity
- Unexplained weight gain or loss despite normal appetite
- Feeling unusually fatigued, even after a good night's sleep
Red-flag signs of cancerous nodules
While most nodules are benign, there are warning signs that deserve a prompt evaluation:
- Rapid growth over weeks
- Persistent pain or tenderness
- Hoarseness that won't improve
- Enlarged lymph nodes in the neck
If any of these pop up, think of it as your body's call 911 button and book an appointment sooner rather than later.
When to Worry
Size thresholds that matter
So, is a 2.5cm thyroid nodule large? Generally, nodules larger than 2cm get a closer look, especially if they have suspicious ultrasound features. A 7mm nodule is often monitored, but if it's hot on a scan (producing excess hormone) it may still need attention.
Size vs. action table
| Size | Typical Management |
|---|---|
| < 1cm | Watchful waiting, repeat US in 1224mo |
| 12cm | Consider FNA if suspicious or patient anxious |
| > 2cm | Recommend Fine-Needle Aspiration (FNA) or surgical consult |
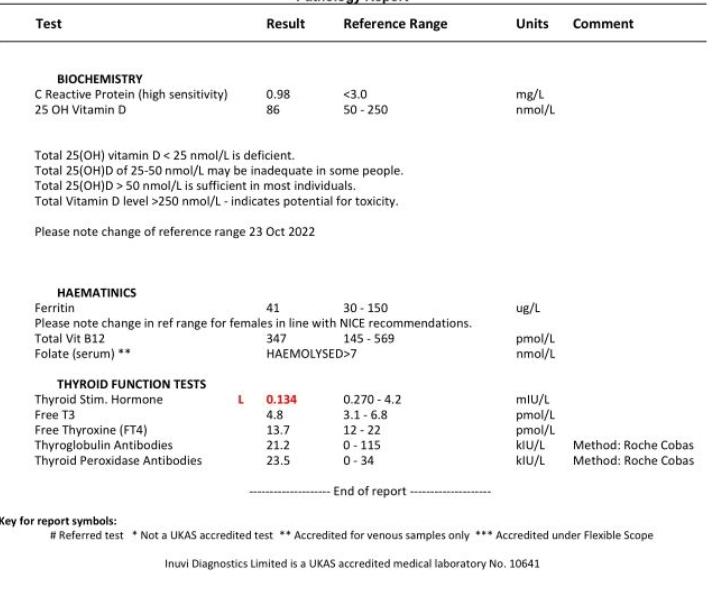
Normal labs, still a concern?
Many wonder, can a thyroid lump be cancerous even with normal labs? Absolutely. A nodule can have normal TSH, T3, and T4 values and still be malignant. Blood tests are great for checking hormone function, but imaging does the detective work. If you suspect thyroid hormone deficiency, it is important to consult with your healthcare provider about appropriate testing and management, as hypothyroidism and related conditions might contribute to symptoms and nodular growth thyroid hormone deficiency.
Risk factors that tip the scale
- Age over 45
- Personal or family history of thyroid cancer
- Radiation exposure to the head/neck (e.g., childhood radiation therapy)
- Male gender (though nodules are more common in women, cancer rates are higher in men)
Expert insight
According to an endocrinology review, the overall risk of malignancy in a thyroid nodule is about 515%, rising sharply when the above risk factors are present.
Diagnosis Process Overview
First-line blood work
Doctors start with a simple panel: TSH, free T4, and occasionally calcitonin (a marker for medullary thyroid cancer). If these are normal, it tells us the gland is still doing its jobeven if a lump is present.
Imaging: the ultrasound tour
High-resolution neck ultrasound is the gold standard. It shows size, composition (solid vs. cystic), and suspicious features like microcalcifications or irregular borders. The American Thyroid Association recommends ultrasound for every palpable nodule.
Fine-Needle Aspiration (FNA)
If the nodule is >1cm or has worrisome ultrasound traits, an FNA is performed. A thin needle extracts cells for cytology. Results are reported using the Bethesda system, ranging from benign (Category II) to malignant (Category VI).
Real-life case snippet
Sarah, a 38-year-old teacher, discovered a 2.8cm lump during a routine checkup. Her labs were perfect, but the ultrasound showed microcalcifications. An FNA confirmed a benign follicular nodule. Knowing the exact nature saved her months of anxiety and a needless surgery.
Treatment Options Overview
Watchful waiting
If the nodule is small, solid, and cytologically benign, most endocrinologists recommend active surveillance. That means a repeat ultrasound every 1218 months to make sure nothing changes.
Medication and hormone suppression
For some benign nodules, low-dose levothyroxine can shrink the growth by lowering TSH stimulation. This approach works best when the nodule is under 2cm and not cystic. Levothyroxine is also the standard therapy for managing primary hypothyroidism, restoring normal thyroid hormone levels and alleviating symptoms related to underactive thyroid function.
Thyroid cyst treatment
Cysts can be drained with a simple needle aspiration. If the cyst refills quickly, a small amount of a sclerosing agent (like ethanol) may be injected to seal it off. Most patients feel relief within days.
Surgical options
When a nodule is malignant, rapidly growing, or causing compressive symptoms (difficulty breathing or swallowing), surgery becomes necessary. There are two main procedures:
- Lobectomy removal of the affected lobe; often enough for low-risk cancers.
- Total thyroidectomy removal of the entire gland; reserved for larger cancers or multinodular disease.
Risks vs. benefits table
| Procedure | Typical Risks | Recovery Time |
|---|---|---|
| Lobectomy | Low risk of vocal cord injury, possible temporary hypocalcemia | 12 weeks |
| Total thyroidectomy | Higher risk of permanent hypocalcemia, need for lifelong thyroid hormone | 24 weeks |
Living With a Lump
Monitoring schedule you can trust
Most clinicians suggest an ultrasound at 612 months after the initial discovery, then yearly if nothing changes. If the nodule grows >20% in any dimension, a repeat FNA is usually recommended.
Diet, lifestyle, and peace of mind
- Maintain adequate iodine intake (seafood, iodized salt) but avoid excess, which can provoke nodule growth.
- Manage stressstress hormones can aggravate thyroid symptoms.
- Practice good neck posture; a forward-head posture can make an existing lump feel more prominent.
Emotional side of the journey
Finding a lump can trigger a wave of what-ifs. You're not alone. Support groups provide a safe space to share fears and celebrate good news.
Personal anecdote
When my own thyroid nodule was discovered, I felt a mix of curiosity and dread. I kept a simple journaldate, size change, any new symptoms. Seeing the steady line on the graph helped calm my mind. Over a year, the nodule stayed the same size, and I learned to treat it as a quiet neighbor rather than a looming threat.
Conclusion
Most thyroid lumps are harmless, but size, symptoms, and personal risk factors dictate when you should act. Keep an eye on any changes, talk openly with a qualified endocrinologist, and follow the recommended imaging schedule if red-flag signs appear. Remember, knowledge is a powerful allyarmed with the right information you can make confident, calm decisions about your health.
Do you have a thyroid lump story or a question you've been holding onto? Share it in the comments below, and let's support each other on the path to wellness.
FAQs
What causes a thyroid lump?
A thyroid lump can develop from benign growths like cysts or solid nodules, iodine deficiency, hormonal changes, or, in rare cases, thyroid cancer.
When should I be concerned about the size of a thyroid lump?
Lumps larger than 2 cm or those that grow quickly, cause pain, or produce hoarseness should be evaluated promptly by a healthcare professional.
Can a thyroid lump be cancerous even if my blood tests are normal?
Yes. Normal TSH, T3, and T4 levels do not rule out cancer; imaging and possibly a fine‑needle aspiration are needed to assess malignancy.
What is the typical follow‑up schedule for a benign thyroid nodule?
Most doctors recommend an ultrasound at 6‑12 months after discovery, then annually if the nodule remains unchanged. Any growth of >20% prompts repeat testing.
Are there non‑surgical treatments for thyroid cysts?
Yes. Simple needle aspiration can drain the fluid, and sometimes a small amount of ethanol is injected to prevent the cyst from refilling.