Primary hypothyroidism is when your thyroid gland itself cant pump enough hormone into your bloodstream. In plain English, its like a thermostat thats stuck on a low setting, leaving your whole body feeling a little too chilly, sluggish, and out of sync.
Below, Ill walk you through what drives this condition, how to spot it, the tests doctors use, and the best ways to get your metabolic furnace back to full powerall backed by realworld experience and trusted medical sources.
Understanding Primary Hypothyroidism
Definition in Plain Language
Think of the thyroid as a tiny, butterflyshaped organ that releases hormones (T4 and T3) to keep your metabolism humming. In primary hypothyroidism, the gland is the problemit's underactive, not the pituitary gland above it.
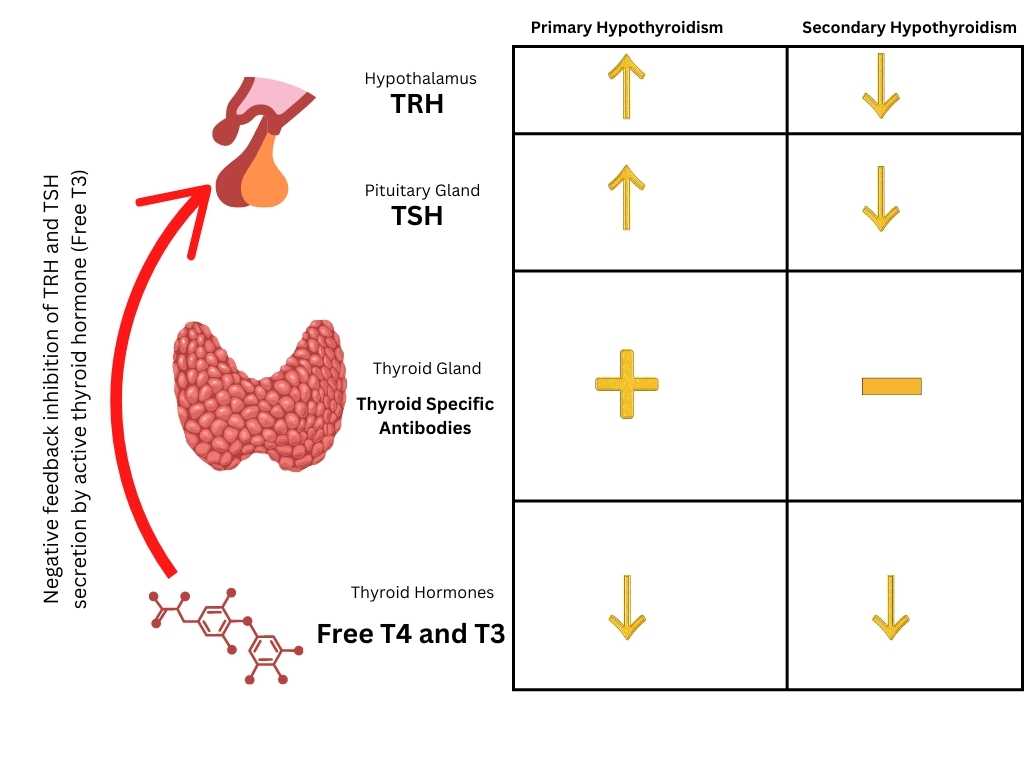
Primary vs. Secondary Quick Comparison
| Aspect | Primary Hypothyroidism | Secondary (Central) Hypothyroidism |
|---|---|---|
| Root Cause | Thyroid gland damage or dysfunction | Pituitary or hypothalamus dysfunction |
| Typical TSH | Elevated (high) | Low or normal |
| Treatment | Levothyroxine (T4) replacement | Often combination T4/T3 or hormonereleasing therapy |
| Common Triggers | Autoimmune (Hashimotos), surgery, radiation | Brain tumors, pituitary surgery, radiation |
Why Primary Matters
When the problem sits in the thyroid, the body responds by cranking up TSH (thyroidstimulating hormone) to try and coax more hormone out. That surge is a key diagnostic clue and why primary hypothyroidism TSH levels appear in so many lab reports.
Root Causes Explained
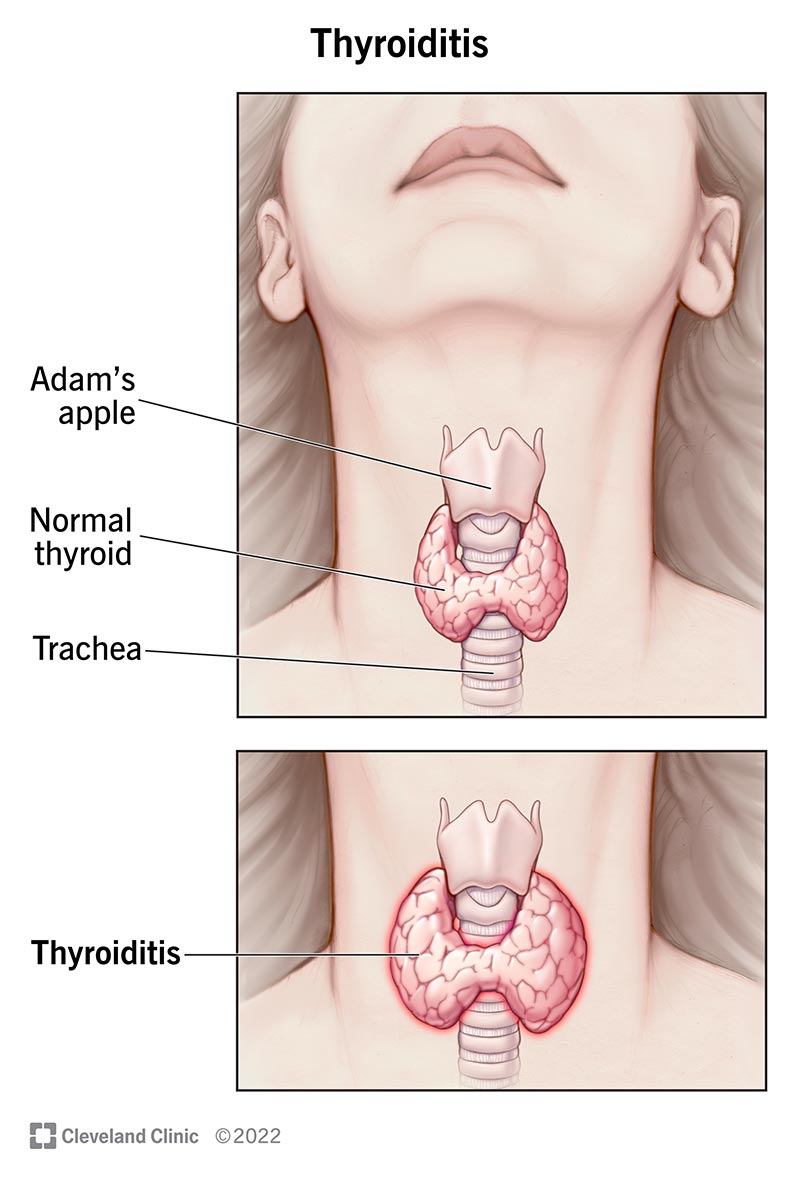
Autoimmune Attack Hashimotos
About 90% of cases stem from Hashimotos thyroiditis, an autoimmune condition where your immune system mistakenly attacks thyroid cells. A friend of mine, Sarah, didnt realize her persistent fatigue was thyroidrelated until a simple blood test revealed high antiTPO antibodies.
Iatrogenic Factors
Sometimes medical treatment itself triggers the condition. Thyroidremoving surgery, radioactive iodine therapy for hyperthyroidism, or even neck radiation for cancer can leave the gland underfunctioning.
MedicationInduced
Drugs like lithium, amiodarone, or interferon can tip the hormonal balance toward hypothyroidism. If youre on any of these, ask your doctor to monitor thyroid function regularly.
Rare Culprits
Congenital defects, infiltrative diseases (e.g., sarcoidosis) or severe iodine deficiency (rare in the U.S.) can also cause primary hypothyroidism, though theyre far less common.
Spotting Common Symptoms
Classic Signs
- Persistent fatigue or feeling heavy
- Unexplained weight gain despite unchanged diet
- Cold intolerance youre the only one shivering in a warm room
- Dry skin, brittle hair, and hair loss
- Constipation and bloating
- Depression or brain fog
Subtle Clues
Sometimes the body whispers before it shouts. Look out for a hoarse voice, irregular menstrual cycles, muscle aches, high cholesterol, or a slowed heart rate. These may be the first hints that your thyroid isnt keeping up.
SelfAssessment Checklist
Print or screenshot this quick list and tick any that sound familiar. If you have three or more, its worth chatting with your doctor about a thyroid screen.
| Symptom | Frequency |
|---|---|
| Fatigue | Daily |
| Weight gain | Gradual |
| Cold sensitivity | Often |
| Dry skin/hair loss | Occasional |
| Depression/brain fog | Recurring |
How Diagnosis Works
Lab Work The Core Trio
The first stop is a blood draw. Doctors look at:
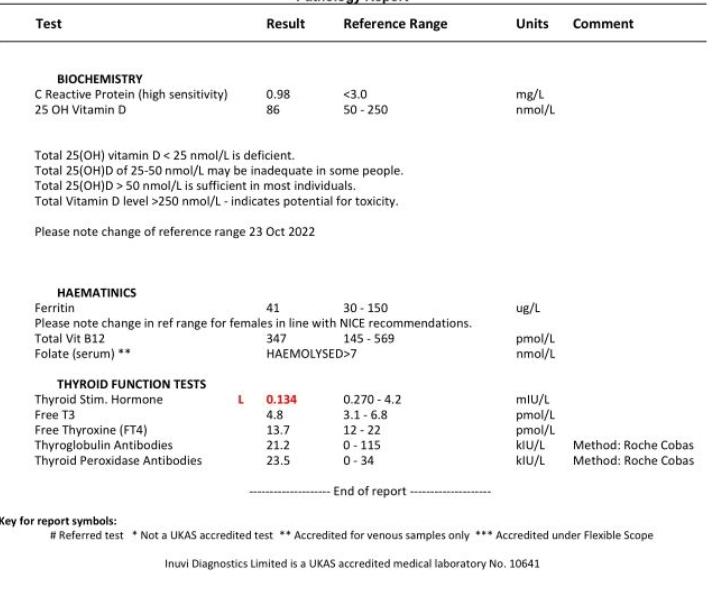
- TSH (ThyroidStimulating Hormone) Elevated levels (>4.0mIU/L) are the hallmark of primary hypothyroidism.
- Free T4 Low levels confirm the thyroid isnt making enough hormone.
- Free T3 Usually normal, but may dip low in severe cases.
According to the , a TSH above 10mIU/L almost always warrants treatment.
Antibody Testing
AntiTPO and antiTG antibodies reveal an autoimmune cause. A positive result strengthens the diagnosis of Hashimotos, guiding both treatment and longterm monitoring.
When Imaging Is Needed
Ultrasound can detect nodules or structural damage, while a radioactive iodine uptake (RAIU) scan helps rule out thyroid autonomy. Most patients dont need imaging unless something feels off.
Ruling Out Secondary Causes
If TSH is low or normal but symptoms persist, doctors may explore secondary hypothyroidism. This involves checking pituitary hormone panels and sometimes MRI of the brain. The distinction matters because treatment approaches differ.
Effective Treatment Options
Levothyroxine The Gold Standard
Levothyroxine (synthetic T4) is the goto medication for over 95% of patients. It mimics the hormone your thyroid cant produce, and the body slowly converts it to T3 where needed.
Dosing basics: Start low (usually 2550g daily) and titrate every 68 weeks based on TSH trends. Take it on an empty stomach, preferably 3060 minutes before breakfast, to improve absorption.
Alternative & Adjunct Therapies
- Liothyronine (T3) Rarely used alone; sometimes added for patients who still feel sluggish despite normal TSH.
- Combination therapy A mix of T4 and T3; the debate is ongoing, but a small subset benefits.
- Desiccated thyroid extract Derived from pig thyroid; not firstline due to dose variability.
Monitoring Success
After the dose stabilizes, your doctor will repeat the TSH after 68 weeks. The goal is a TSH within the reference range (often 0.52.5mIU/L for most adults). Keep a symptom journal; numbers are useful, but how you feel matters more.
Risks of Overtreatment
Too much thyroid hormone can cause heart palpitations, anxiety, sleep disturbances, and even bone loss over time. Thats why regular labs and honest communication with your provider are key.
Primary vs. Secondary
Key Differences at a Glance
| Feature | Primary | Secondary |
|---|---|---|
| Origin | Thyroid gland | Pituitary/hypothalamus |
| TSH Level | High | Low/Normal |
| T4 Level | Low | Low |
| Treatment | Levothyroxine | Hormonereleasing therapy, sometimes surgery |
When Misdiagnosis Happens
If a patients TSH is normal but symptoms linger, clinicians might miss secondary hypothyroidism. Redflag clues include a history of pituitary surgery, radiation, or unexplained low ACTH levels. Always ask your doctor about the full differential if you feel something isnt adding up.
ICD10 Coding Info
Primary Code
The standard diagnosis code for unspecified primary hypothyroidism is E03.9. This is what youll see on most lab reports and insurance claims.
When to Use SubCodes
- E03.0 Postprocedural hypothyroidism (after thyroid surgery)
- E03.2 Hypothyroidism due to iodine deficiency
- E03.8 Other specified hypothyroidism
Accurate coding ensures proper reimbursement and helps health systems track disease prevalence.
ThyroidFriendly Lifestyle
Nutrition Basics
While diet cant replace medication, certain nutrients support thyroid health:
- Iodine Essential for hormone synthesis. Sources: iodized salt, seaweed (in moderation).
- Selenium Helps convert T4 to T3. Brazil nuts, sunflower seeds.
- Zinc Important for hormone production. Beef, pumpkin seeds.
Foods to Approach With Caution
Large amounts of soy, cruciferous vegetables (broccoli, cabbage) and gluten (if you have celiac disease) can interfere with hormone absorption. That doesnt mean you must ditch them entirelyjust enjoy them cooked and in reasonable portions.
Sample ThyroidFriendly Meal
Breakfast: Greek yogurt with a handful of Brazil nuts, a drizzle of honey, and a slice of wholegrain toast.
Lunch: Grilled salmon (rich in selenium) on a mixedgreen salad with olive oil.
Dinner: Stirfried chicken with bell peppers, carrots, and a side of quinoa.
Snacks: Apple slices with almond butter.
Exercise & Stress Management
Regular, moderate activitythink brisk walks, yoga, or swimmingboosts metabolism and combats weight gain. Stress hormones (cortisol) can worsen hypothyroid symptoms, so practices like mindfulness or deep breathing are worth the time.
Supplements: Do They Help?
Only take supplements if youre deficient. A study in the found that selenium supplementation modestly improved antiTPO antibodies but didnt replace hormone therapy.
When to Seek Help
RedFlag Symptoms
- Rapid weight gain (more than 5kg in a month)
- Severe swelling of the face or extremities (myxedema)
- Chest pain, irregular heartbeat, or fainting
- Extreme fatigue that interferes with daily life
If any of these appear, call your provider right away; they could signal an acute worsening that needs prompt attention.
Routine FollowUp Schedule
After starting or adjusting medication, check TSH every 68 weeks until stable. Once your levels are steady, an annual test is usually enoughunless you become pregnant, start new medications, or notice symptom changes.
Finding the Right Specialist
Look for boardcertified endocrinologists or primarycare doctors with a strong background in thyroid disorders. Many clinics list physician credentials on their websites; dont hesitate to ask about their experience with hypothyroidism.
Conclusion
Primary hypothyroidism is common, but it doesnt have to control your life. By recognizing the symptoms, getting the right labs, and partnering with a knowledgeable clinician, you can restore balance with a simple daily pill, mindful nutrition, and a bit of selfcare. If you suspect your thyroid is acting up, schedule a blood test and start the conversationyour body will thank you.
Got a story about managing hypothyroidism, or a question thats still lingering? Drop a comment below. Were in this together, and sharing our experiences makes the journey a little less messy.
FAQs
What are the most common symptoms of primary hypothyroidism?
Typical signs include persistent fatigue, weight gain, cold intolerance, dry skin, hair loss, constipation, depression, and slowed heart rate.
How is primary hypothyroidism diagnosed?
Diagnosis starts with blood tests measuring TSH (usually elevated) and free T4 (low). Antibody tests for anti‑TPO and anti‑TG help identify Hashimoto’s, the most common cause.
What is the first‑line treatment for primary hypothyroidism?
The standard therapy is levothyroxine, a synthetic form of T4, taken on an empty stomach. Doses are adjusted every 6–8 weeks until TSH is within the target range.
Can diet or supplements replace medication for primary hypothyroidism?
Diet and supplements can support thyroid health but cannot replace hormone replacement. Iodine, selenium, and zinc are beneficial, while excessive soy or cruciferous veggies may interfere with absorption.
When should I seek urgent medical care for hypothyroidism?
Urgent care is needed for rapid weight gain, severe swelling (myxedema), chest pain, irregular heartbeat, fainting, or extreme fatigue, as these may signal a thyroid crisis.