Quick answer: if your thyroid is overactive, youre more likely to lose bone density and develop osteoporosisand certain thyroid medications can tip the balance, too.
Why it matters: knowing how these two systems interact helps you catch problems early, have a smarter conversation with your doctor, and choose treatments that protect both your thyroid and your bones.
Thyroid Hormones & Bones
What is bone remodeling and why thyroid matters?
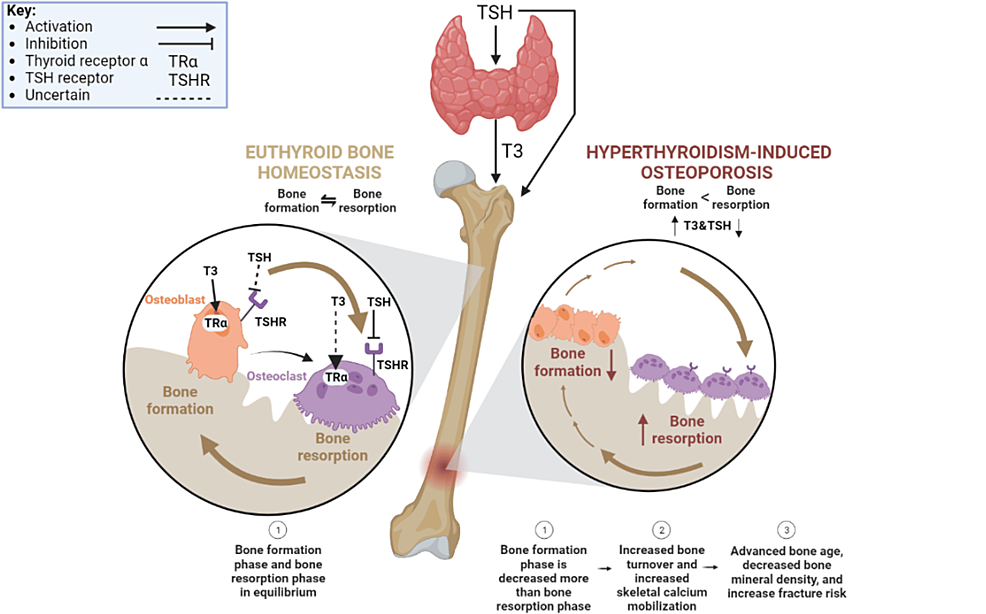
Our skeleton isnt a static structure; its constantly being torn down and rebuilt in a process called remodeling. Osteoclasts chew away old bone, while osteoblasts lay down fresh material. Thyroid hormones, especially T3, act like a fastforward button on this cycle. When levels are too high, bone is broken down faster than it can be rebuilt, leading to loss of density.
Overt vs. Subclinical Hyperthyroidism
Not all hyperthyroidism looks the same. Overt hyperthyroidism shows obvious symptomsweight loss, rapid heartbeat, heat intolerancewhile subclinical hyperthyroidism often hides behind normal thyroidstimulating hormone (TSH) levels but slightly elevated T3/T4. Both can affect bones, but the risk is steeper with overt disease.
Comparison of Bone Impact
| Condition | BoneDensity Change | Fracture Risk | Typical Lab Values |
|---|---|---|---|
| Overt Hyperthyroidism | 510% in 12years | 23 higher | Low TSH, high Free T4/T3 |
| Subclinical Hyperthyroidism | 24% in 35years | 1.5 (postmenopausal women) | Lownormal TSH, normal Free T4/T3 |
The role of subclinical hyperthyroidism in osteoporosis risk
Recent research (a 2023 study in ) shows that even mild, undetected overactivity can shave away a few percent of bone each year, especially in women after menopause. Thats why many endocrinologists now recommend a DEXA scan when TSH drops below 0.4IU/mL.
Symptoms That Connect
Typical hyperthyroidism signs that may mask bone loss
When you think of an overactive thyroid you probably picture a racing heart, shaky hands, and feeling on fire. Those are the classic hyperthyroidism symptoms. But bone pain can creep in toooften described as an ache in the lower back or hips. Its easy to write that off as just growing older, when in fact the thyroid may be driving it.
Early bonerelated clues you shouldnt ignore
Pay attention if you notice:
- Unexplained joint or hand pain
- Frequent minor fractures from lowimpact falls
- A subtle loss of height over months
These signs, combined with thyroid issues, should raise a red flag.
When to suspect a thyroidbone connection
Heres a quick checklist you can keep on your fridge:
- Diagnosed hyperthyroidism (any form)
- Bone pain or fracture history without obvious cause
- Taking levothyroxine or antithyroid meds for>2years
- Family history of osteoporosis
If three or more apply, talk to your doctor about a bonedensity test.
Medication Impacts
Does levothyroxine cause osteoporosis?
Levothyroxine is a lifesaver for hypothyroidism, but when the dose overshoots, it mimics hyperthyroidism. High doses suppress TSH, accelerating bone turnover. A classic review from the American Academy of Family Physicians notes that patients on highdose levothyroxine have a modest increase in fracture risk, especially if theyre postmenopausal women.
Can hypothyroidism cause osteoporosis?
In most cases, an underactive thyroid actually slows bone turnover, which can be protective. The bigger risk comes from overtreatmentwhen doctors give too much levothyroxine, the body ends up in a hyperstate. So its less the disease itself, more the medication dosage that matters. If youre comparing replacement options, some patients research Armour vs levothyroxine to understand differences in symptom control and dosing approaches that might influence bone health.
Hashimotos and osteoporosis
Hashimotos is an autoimmune attack on the thyroid that often leads to hypothyroidism. While the disease alone isnt a direct bonethreat, many patients with Hashimotos are on levothyroxine, so the dosage question reemerges. Some clinicians also observe that chronic inflammation can subtly affect bone health, so keeping inflammation in check (through diet or medication) may be wise.
Managing bone health while on thyroid medication
Heres a simple pillandplate plan:
- Take levothyroxine on an empty stomach, 30minutes before breakfast.
- Get a baseline DEXA scan within 6months of starting treatment.
- Include calciumrich foods (dairy, leafy greens) and vitaminD (sunlight, fortified foods). The recommended daily intake is about 1,200mg calcium and 8001,000IU vitaminD for adults over 50.
- Schedule TSH checks every 612months; adjust dose before bone loss becomes a problem.
Diagnosis & Monitoring
Recommended screening protocols
Most guidelines suggest a DEXA scan for anyone with:
- Diagnosed hyperthyroidism for more than 2years
- Subclinical hyperthyroidism with TSH<0.4IU/mL
- Age>50years (or>40years for men)
Think of the scan as a bone selfie that lets you track changes over time.
Interpreting lab results
When you get your labs, look for three pieces:
- TSH the master switch; low levels signal overactivity.
- Free T4/T3 confirm how much hormone is actually circulating.
- Bone turnover markers (like CTX or P1NP) theyre not routine but can help when the picture is blurry.
Red flags that demand specialist referral
If you see any of the following, ask for an endocrinology consult:
- Fracture from a fall that wouldnt normally break a bone
- Rapid decline in bone density (>5% loss in a year)
- Persistent TSH<0.1IU/mL despite medication adjustments
Treatment Strategies
Firstline thyroid treatments that are bonefriendly
Radioactive iodine (RAI) can be a good option because it eliminates overproduction without longterm high hormone levels. Antithyroid drugs (like methimazole) also control hormone output, but they require careful dose monitoring to avoid swinging into hypothyroidism.
Pharmacologic options for osteoporosis in thyroid patients
If bone loss is already evident, doctors may add:
- Bisphosphonates (e.g., alendronate) proven to reduce fracture risk.
- Denosumab a monoclonal antibody that works well for people who cant tolerate bisphosphonates.
- Selective estrogen receptor modulators (SERMs) useful especially for postmenopausal women.
These medicines dont interfere with thyroid treatment, but they should be coordinated with your endocrinologist.
Lifestyle hacks that help both thyroid and bone health
Heres the triplewin checklist:
- Nutrition: Aim for iodinerich foods (seaweed, fish) for thyroid support, and calcium/vitaminD for bone strength.
- Exercise: Weightbearing activitieswalking, dancing, light resistance trainingstimulate bone formation.
- Stress reduction: Chronic stress spikes cortisol, which can hurt bone. Try yoga, deep breathing, or a simple daily walk.
Even small changes add up; think of them as daily votes for a healthier skeleton.
Patientcentered decisionmaking checklist
Before you sign off on any treatment, ask yourself:
- Do I understand the benefits and potential bonerelated side effects?
- Has my doctor explained how well monitor my bone density?
- Am I comfortable with the lifestyle adjustments the plan requires?
- Do I have a clear followup schedule?
RealWorld Stories
Case A: Graves disease and rapid bone loss
Maria, 52, was diagnosed with Graves disease two years ago. Within six months, her DEXA scan showed a 7% drop in lumbar spine density. After switching from propranolol to a lower dose of methimazole and starting calcium/vitaminD supplements, her bone loss slowed dramatically. I felt like I was fighting a doublebattle, she says, but the teamwork between my endocrinologist and my primary doctor saved my spine.
Case B: Longterm levothyroxine and low BMD
John, 60, has been on levothyroxine 125g daily for hypothyroidism for 15years. A routine DEXA revealed osteopenia. His doctor reduced the dose to 88g, rechecked TSH, and added a weekly bisphosphonate. Six months later, his boneturnover markers dropped, and there was a modest gain in bone density. I never imagined my thyroid pill could affect my hips, John laughs, but now Im more careful about the dosage.
Key Takeaways
The connection between thyroid function and bone health is real, bidirectional, and often overlooked. Overactive thyroid stateseven the subtle subclinical kindcan speed up bone loss, while overtreatment of hypothyroidism can create the same problem. By staying alert to symptoms, getting regular bonedensity checks, and working closely with your healthcare team, you can protect both your thyroid and your skeleton.
Feeling empowered? Talk to your doctor about a DEXA scan, review your thyroid medication doses, and add some weightbearing activity to your weekly routine. If youve experienced a similar journey, share your story in the commentsyour experience might be the hint someone else needs to safeguard their bones.
FAQs
Can hyperthyroidism cause osteoporosis?
Yes. Excess thyroid hormones increase bone turnover, leading to faster bone loss and a higher risk of osteoporosis.
What TSH level triggers a DEXA scan?
Guidelines often recommend a DEXA when TSH falls below 0.4 µIU/mL, especially in post‑menopausal women.
Does levothyroxine increase fracture risk?
High‑dose levothyroxine can suppress TSH and mimic hyperthyroidism, modestly raising fracture risk if not properly monitored.
Which osteoporosis medicines are safe with thyroid treatment?
Bisphosphonates, denosumab, and SERMs can be used alongside thyroid meds; coordination with an endocrinologist is advised.
What lifestyle changes help both thyroid and bone health?
Eat iodine‑rich foods, ensure adequate calcium and vitamin D, and do regular weight‑bearing exercise to support both systems.