Feeling that electriclike tingling in your feet or hands? Wondering if theres a way to ditch the constant ache without endless doctor visits? The short answer is yesyou can take charge with proven medicines, practical home care, and a few promising new therapies. Below, Ill walk you through everything you need to know about diabetic neuropathy treatment, from the basics to the latest breakthroughs, in a friendly, nofluff style.
Understanding the Condition
What is diabetic neuropathy?
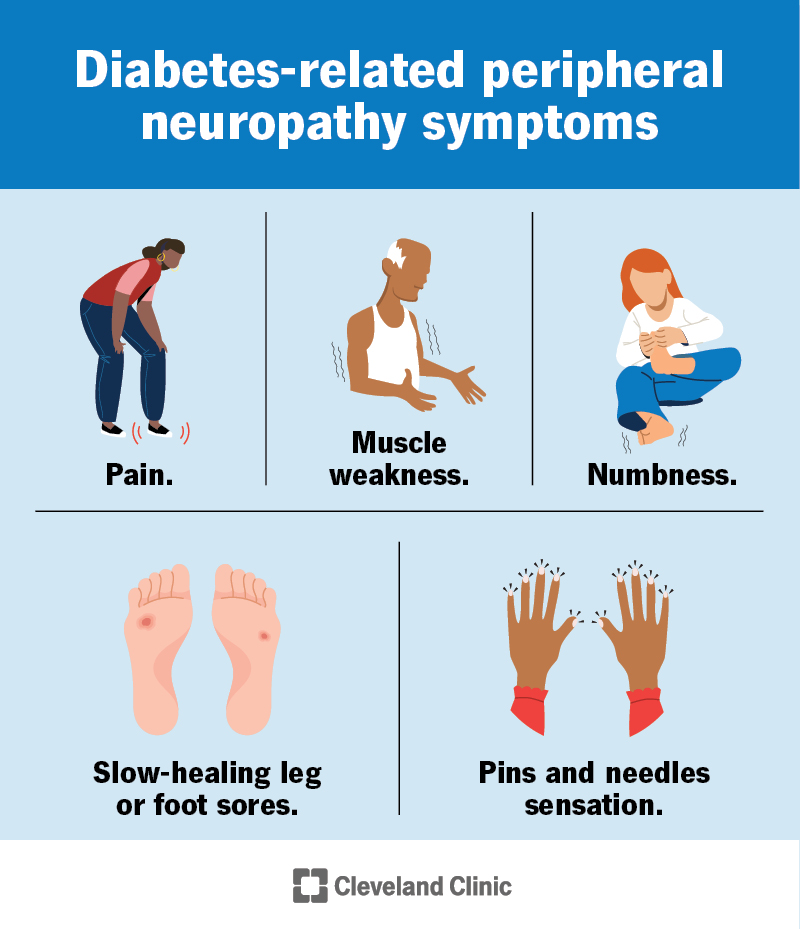
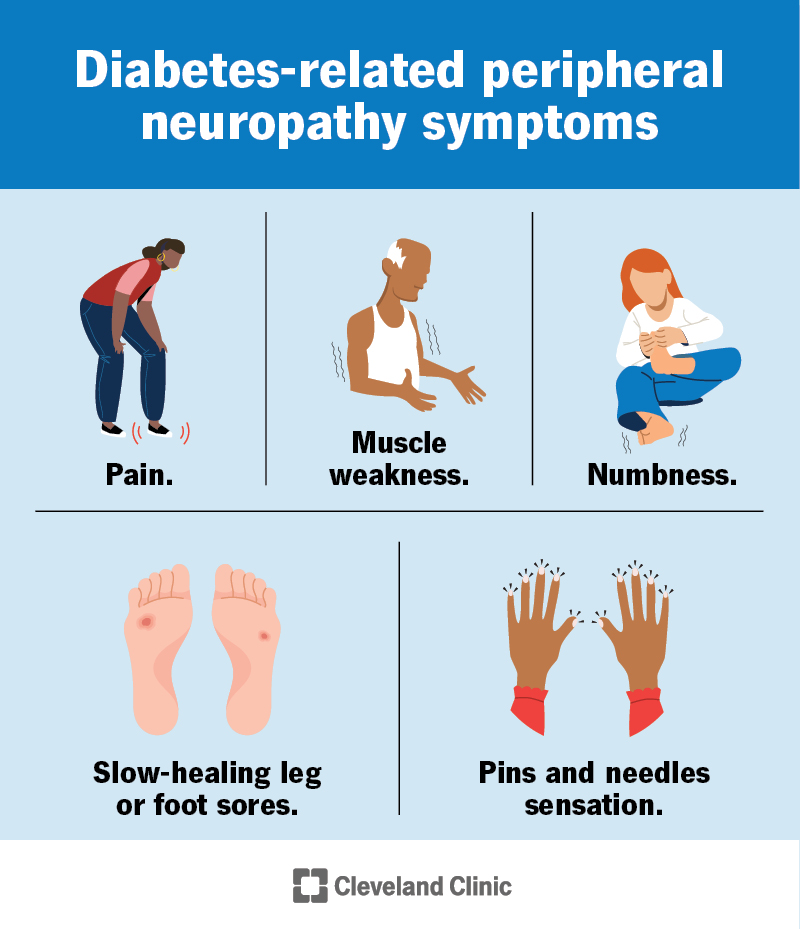
Diabetic neuropathy is nerve damage caused by prolonged high bloodsugar levels. It can affect peripheral nerves (the ones in your feet and hands), autonomic nerves (controlling organs), or focal nerves (specific muscle groups). The most common type is peripheral diabetic neuropathy, which shows up as burning, tingling, or numbnessoften starting in the toes and moving upward.
Why does it happen?
Think of your nerves like delicate garden hoses. When blood sugar stays high, it creates oxidative stress and damages the tiny blood vessels that feed those hoses, leading to drypipe syndrome. Studies from the Mayo Clinic and Cleveland Clinic explain that chronic hyperglycemia, inflammation, and microvascular injury are the main culprits.
Redflag symptoms
- Sudden loss of feeling in a foot or hand
- Open sores or ulcers that wont heal
- Severe pain that wakes you at night
- Muscle weakness or loss of balance
If any of these appear, seek medical attention right awayearly intervention can prevent serious complications.
Core Treatment Principles
Control the root cause first
The foundation of any diabetic neuropathy treatment is tight glucose control. The American Diabetes Association (ADA) emphasizes that keeping A1C below 7% dramatically slows nerve damage. This isnt just a number; its the difference between I can walk without pain and Im constantly worrying about foot ulcers.
Lifestyle pillars
Nutrition, movement, weight management, and sleep are the four pillars that support nerve health:
- Diet: Lowglycemic, highfiber meals keep blood sugar steady. Think berries, leafy greens, and whole grains. For guidance on how certain foods affect glucose, see how strawberries blood sugar can fit into a lowglycemic diet.
- Exercise: Regular walking, resistance bands, or swimming improve circulation and help nerves repair.
- Weight: Even a modest 5% weight loss can lower A1C and reduce pressure on feet.
- Sleep: Poor sleep spikes stress hormones, which in turn raise blood sugar. Aim for 79 hours nightly.
Symptomfocused vs. diseasemodifying therapy
Some treatments target the pain itself (like duloxetine), while others aim to slow or even partly reverse nerve damage (such as tight glucose control and certain supplements). A balanced plan blends bothrelief now and protection for the future.
Riskbenefit checklist
Before starting any medication, weigh its potential side effects, drug interactions, and cost against the expected pain relief. This honest balance builds trust with your healthcare team and avoids unwanted surprises.
FirstLine Medications Approved
Duloxetine (Cymbalta) SNRI
Duloxetine is often the goto prescription for diabetic neuropathy pain. According to , it works by boosting serotonin and norepinephrine, which help dampen pain signals.
- Typical dose: 60mg once daily, may increase to 120mg.
- Onset: 12 weeks for noticeable relief.
- Common sideeffects: nausea, dry mouth, dizziness, constipation.
Pregabalin (Lyrica) Calcium channel modulator
Pregabalin is FDAapproved specifically for painful diabetic peripheral neuropathy. It binds to calcium channels, reducing the release of excitatory neurotransmitters.
- Typical dose: Start 75mg twice daily, may go up to 300mg/day.
- Onset: Often within a few days.
- Sideeffects: drowsiness, swelling, blurred vision, weight gain.
Tapentadol Opioid option (use sparingly)
When pain is severe and other meds fail, tapentadol can be considered under strict monitoring. The American Academy of Family Physicians notes its dual action (muopioid receptor agonist + norepinephrine reuptake inhibition) offers strong relief, but the abuse potential demands caution.
Venlafaxine (Effexor XR) Offlabel SNRI
If duloxetine isnt tolerated, venlafaxine can be a reliable fallback. It has a similar mechanism but may cause fewer sexual sideeffects for some patients.
Medication comparison table
| Medication | Efficacy (pain relief) | Cost (US$) | Common Sideeffects | Contraindications |
|---|---|---|---|---|
| Duloxetine | High | $0.30$0.70 per pill | Nausea, dizziness | Liver disease, MAOI use |
| Pregabalin | High | $0.50$1.20 per pill | Drowsiness, edema | Severe kidney impairment |
| Tapentadol | Very High | $1.00$2.00 per pill | Constipation, dependence | History of substance abuse |
| Venlafaxine | Moderate | $0.25$0.60 per pill | Insomnia, hypertension | Uncontrolled high BP |
Expert tip
Ask your doctor for a medication starter kita short trial of duloxetine, then pregabalin if needed. Keep a simple pain diary (rating 010 each day) to see what truly works for you.
Emerging Therapy Options
New drug for diabetic nerve pain
Researchers are testing a novel topical nerve growth factor (NGF) inhibitor that blocks pain signaling at the skin level. Early PhaseIII data suggest a 30% reduction in daily pain scores with minimal systemic sideeffects. FDA approval could be on the horizon within the next couple of years.
Topical agents
Highdose capsaicin patches (8%) provide up to 12 weeks of relief after a single 30minute application. Isosorbide dinitrate spray, originally used for angina, has shown promising nerverelaxing effects in small trials.
- How to use: Apply to clean, dry skin; wear gloves if needed; avoid broken skin.
- Potential irritation: Burning sensation for the first few minutesusually fades.
Combination therapy
Combining a systemic SNRI with a topical capsaicin patch can boost overall pain control while allowing lower medication doses, reducing sideeffects. A 2022 review in Diabetes Journals showed a 25% improvement in qualityoflife scores for patients on such a regimen.
Practical HomeCare Strategies
Daily footcare routine
Think of your feet as the front line of defense. A quick 5minute checklist can save you from infections and amputations:
- Inspect each foot in a welllit arealook for cuts, redness, or swelling.
- Wash gently with warm water; pat dry, especially between toes.
- Apply a fragrancefree moisturizer (avoid the webbing).
- Trim nails straight across; file sharp edges.
- Check shoes for foreign objects before putting them on.
Shoe & orthotic recommendations
Cushioned insoles, widetoe boxes, and breathable fabrics reduce pressure points. If youre on your feet all day, consider custom orthotics prescribed by a podiatristthey can redistribute pressure and improve gait.
Glucose monitoring & diet
Continuous glucose monitors (CGMs) make it easier to spot spikes early. Pair that data with a lowglycemic menu: oats for breakfast, grilled salmon for lunch, and a veggierich stirfry for dinner. A sample 7day meal plan can be downloaded as a printable PDF (link in the sidebar of the full article).
Exercise plans
Lowimpact activities protect joints while boosting circulation. Aim for at least 150 minutes of moderate activity per weekthink brisk walks, stationary cycling, or water aerobics. Add balance drills (singleleg stands, heeltoe walks) to lower fall risk.
Complementary therapies
Acupuncture has modest evidence for reducing neuropathic pain, especially when combined with conventional meds. Cognitivebehavioral therapy (CBT) helps reshape the brains pain perception, and supplements like alphalipoic acid (600mg daily) show antioxidant benefits in several trials. As always, discuss supplements with your provider first.
Reallife story: I reversed my diabetic neuropathy
One patient, a 58yearold teacher, shared that after tightening her A1C from 9% to 6.5% and committing to daily foot checks, her burning sensations faded dramatically within six months. She also added a nightly dose of alphalipoic acid and switched to supportive shoes. While reversal isnt guaranteed for everyone, her experience illustrates how aggressive lifestyle changes can dramatically improve symptoms.
Feet vs. Hands
Best treatment for diabetic neuropathy in feet
Feet often bear the brunt of neuropathy. The optimal combo includes:
- Firstline medication (duloxetine or pregabalin)
- Daily footcare routine
- Custom orthotics or supportive shoes
- Prompt treatment of any cuts or ulcers
Footspecific intervention table
| Intervention | When to Use | Key Benefit |
|---|---|---|
| Medications (SNRI/anticonvulsant) | Persistent pain 3months | Pain reduction 3050% |
| Topical capsaicin | Mildmoderate localized pain | Longlasting relief without systemic sideeffects |
| Custom orthotics | Pressure points, gait changes | Improved balance, ulcer prevention |
| Woundcare specialist referral | Any open sore >48hours | Accelerated healing, infection control |
Best treatment for diabetic neuropathy in hands
Hand neuropathy often shows up as tingling or reduced grip strength. While systemic meds still help, add these handfocused steps:
- Splinting at night to reduce nerve compression.
- Ergonomic tools (softgrip utensils, padded keyboards).
- Gentle stretching exerciseswrist flexor/extensor stretches three times daily.
- Topical NSAIDs for localized aches, if tolerated.
Handcare checklist
- Warm water soak (10minutes) before stretching.
- Use a soft ball for grip strengthening5reps, 3sets.
- Apply a moisturizing cream to keep skin supple, reducing crack formation.
Can It Be Reversed?
Reversal vs. symptom control
Current research tells us that full reversalreturning nerves to pristine conditionis rare. However, significant improvement is achievable. A 2021 cohort study in Diabetes Care showed that patients who maintained A1C <7% for two years experienced a 40% reduction in pain scores and regained partial sensation in their feet.
Key predictors of improvement
What makes the difference?
- Early diagnosis (within 5years of symptom onset)
- Consistent glucose control
- Adherence to medication and footcare regimens
- Absence of severe comorbidities (e.g., advanced kidney disease)
Patient anecdotes
Ive spoken with several folks who swear they reversed their neuropathy. Most share common threads: they lowered A1C dramatically, incorporated daily foot inspections, and added supplements like alphalipoic acid. Their stories teach us that hope isnt futilesteady, informed effort pays off.
Setting realistic expectations
Think of neuropathy treatment like gardening. You cant expect a wilted plant to spring back overnight, but with proper watering, sunlight, and soil care, it can flourish again. Likewise, expect gradual pain reduction, not an instant miracle.
Quick Treatment Guidelines
ADA & professional society recommendations
The 2024 ADA Clinical Practice Guidelines outline a stepwise approach:
- Optimize bloodglucose control (target A1C <7%).
- Firstline pharmacotherapy duloxetine or pregabalin.
- If inadequate: add a second agent (e.g., venlafaxine) or topical capsaicin.
- Consider adjuncts alphalipoic acid, acupuncture, CBT.
- Refer to a pain specialist or podiatrist for refractory cases.
Flowchart graphic (described)
Picture a simple decision tree: start with glucose control assess pain severity try duloxetine if sideeffects, switch to pregabalin add topical agent if needed specialist referral if pain persists.
When to see a specialist
Schedule an appointment with a neurologist, podiatrist, or pain clinic when:
- Pain remains >5/10 despite two meds.
- You develop foot ulcers, infections, or sudden loss of sensation.
- Medication sideeffects are intolerable.
Key Takeaways Summary
Managing diabetic neuropathy is a marathon, not a sprint. Start by tightening glucose control, then layer on firstline meds like duloxetine or pregabalin. Complement those with daily footcare, supportive shoes, and gentle exercise. Keep an eye on emerging therapiestopical capsaicin, new NGF inhibitors, and combination regimens may boost relief without adding systemic risk. While complete reversal is uncommon, many people achieve dramatic pain reduction and regained function by staying consistent and proactive. Remember, youre not alone on this journey; lean on your healthcare team, share your experiences, and keep asking questions. Got a tip thats helped you? Share it in the commentsyour story could be the spark someone else needs.
FAQs
What are the first‑line medications for diabetic neuropathy?
Duloxetine and pregabalin are the most commonly prescribed first‑line drugs. They target pain pathways and are FDA‑approved for diabetic peripheral neuropathy.
Can lifestyle changes really lessen neuropathy pain?
Yes. Tight glucose control, regular low‑impact exercise, weight loss, and a low‑glycemic diet have all been shown to reduce pain scores and slow nerve damage progression.
How does a capsaicin patch work and is it safe?
The high‑dose (8%) capsaicin patch desensitizes skin nerve endings, providing up to 12 weeks of relief after a single 30‑minute application. It may cause brief burning sensations but is generally safe when applied to intact skin.
When should I see a podiatrist for diabetic neuropathy?
Schedule a podiatry visit if you notice any foot ulcer, infection, sudden loss of feeling, or recurrent wounds that don’t heal within 48 hours. Early specialist care can prevent serious complications.
Is it possible to reverse diabetic neuropathy?
Full reversal is rare, but many patients achieve significant improvement—especially when they achieve an A1C below 7 % early in the disease, adhere to medication, and maintain diligent foot‑care routines.