Cervical stroma MRI shows the lowsignal T2 ring that surrounds the cervix; any break in this ring signals possible stromal invasion, a crucial finding for cancer staging.
Understanding how that tiny dark ring looks on an exam can be the difference between a confident treatment plan and a lot of secondguessing. In the next few minutes well walk through what normal looks like, how cancer changes the picture, the best way to scan it, and what those images mean for realworld decisions. Grab a coffee, and lets dig inno medical jargon firehose, just friendly explanations.
Cervical Anatomy
Normal cervix on MRI
On T2weighted images the cervix is a layered structure. The innermost canal (the endocervical canal) appears bright because of mucus, while the surrounding musclerich tissue the cervical stroma is dark, almost like a thin ink line. On T1 its a little less dramatic, but the stroma still stays relatively lowsignal. The key thing to remember is that the stroma forms a continuous, lowsignal ring that hugs the bright canal.
Quick reference
| Layer | T1 Signal | T2 Signal |
|---|---|---|
| Endocervical canal (mucus) | Iso or slightly hyperintense | Hyperintense (bright) |
| Cervical stroma | Lowtointermediate | Low (dark) |
| Parametrial fat | High | High |
Why the stroma matters
If the dark ring stays smooth and unbroken, we usually assume theres no tumor crossing into the surrounding tissue. Once a tumour breaches that line, the signal becomes irregular you might see a focal bulge, spicules, or a patch where the darkness disappears. That break is the radiologic hallmark of stromal invasion and directly feeds into FIGO staging.
Common pitfalls
- Postmenopausal thinning the ring can look a bit less robust, but its still continuous.
- Blood or mucus pooling can mimic a break, so always scroll through multiple planes.
- Motion artefacts a shaky patient can make a perfect ring look jagged.
Stroma in Cancer
How tumours distort the ring
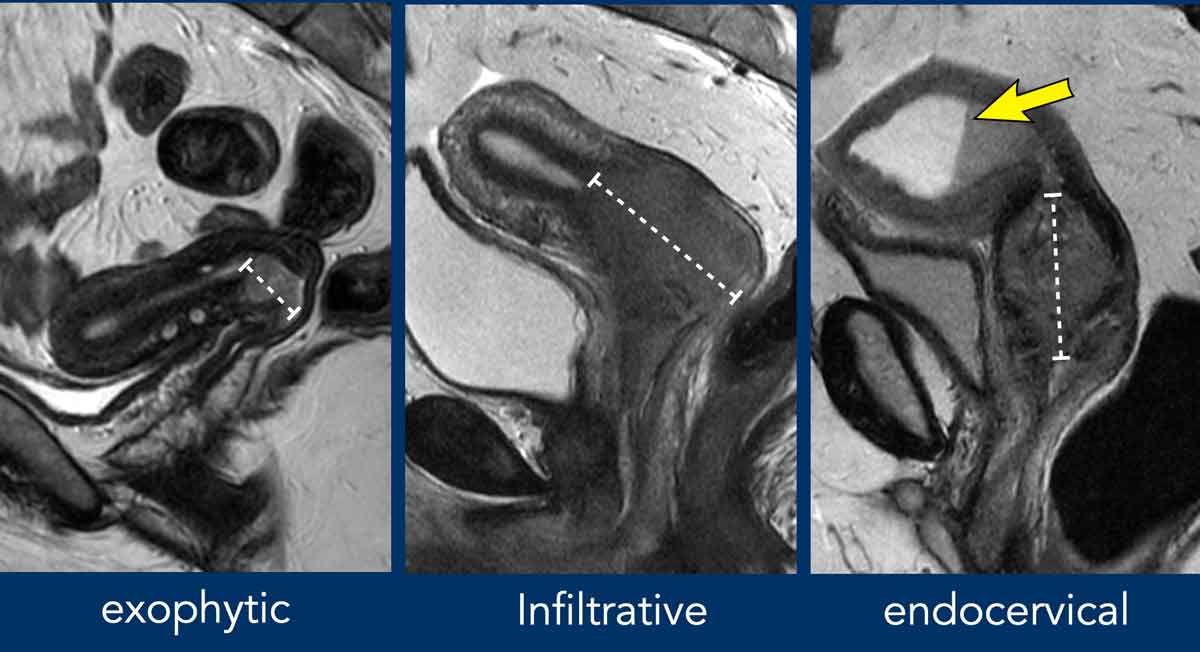
When cancer spreads, it generally starts as a T2hyperintense mass pushing against that lowsignal border. The first sign of invasion is a loss of continuity: a gap, an irregular edge, or a spike reaching into the parametrial fat. In many radiology textbooks youll see sidebyside pictures where one line is smooth, the other has a clear notch that notch tells the surgeon the tumour has gone beyond the cervix.
Illustrative example
Imagine youre looking at a crosssection of a tree trunk. The bark (our stroma) is a uniform dark ring. If a worm (the tumour) bores a tunnel, youll see a distinct hole in the bark. The same visual logic applies on MRI.
Staging basics (FIGO2018)
The International Federation of Gynecology and Obstetrics (FIGO) uses MRI to separate stages I through IV based largely on stromal and parametrial involvement:
| FIGO Stage | MRI Criteria |
|---|---|
| IA | Microinvasion no visible stromal break on MRI. |
| IB | Lesion confined to cervix, intact stromal ring. |
| IIA | Loss of stromal continuity, but no parametrial fat invasion. |
| IIB | Disruption of stromal ring+parametrial fat involvement. |
| IIIAIIIC | Extension to the vagina or pelvic lymph nodes (often need PET/CT). |
| IV | Adjacent organ invasion (bladder, rectum) visible on MRI. |
How reliable is MRI?
Recent systematic reviews report a sensitivity of 92100% and specificity around 7495% for detecting stromal invasionpretty solid numbers, especially when you pair the scan with a skilled radiologist. highlighted that, in expert hands, MRI is the goldstandard for local staging of cervical cancer.
When MRI alone isnt enough
Occasionally, inflammation, recent biopsies, or large leiomyomas can give falsepositive breaks. In those cases, its wise to bring in a second imaging modalitylike PET/CT for nodal assessment or a highresolution transvaginal ultrasound for clarification. The key is to avoid overstaging, which could push a patient toward unnecessarily aggressive treatment.
MRI Protocol
Essential sequences
Think of the protocol as a recipe: you need the right ingredients (sequences) and the right timing (contrast phases). For cervical stroma evaluation, most centres use:
- T2weighted sagittal, axial, and coronal (highresolution, 3mm slices).
- DWI/ADC to assess cellularity tumours are usually bright on highb DWI.
- Dynamic contrastenhanced (DCE) series early arterial phase can highlight parametrial extension.
- Optional T1weighted for fat saturation and to spot hemorrhage.
Tips for a crisp stromal view
1. Use a small fieldofview (20cm) centered on the pelvis.
2 2. Fill the bladder moderately it pushes the uterus up and reduces artefacts.
3 3. Apply fatsuppression on the T2 and DWI to improve contrast between the dark stroma and surrounding fat.
4 4. Keep the patient still; a biteguard or gentle coaching helps.
Common technical slipups
- Too thick slices youll miss subtle interruptions.
- Inadequate coil coverage the pelvic phasedarray coil yields the best signaltonoise.
- Late contrast timing the washout phase can hide early parametrial spread.
Reporting the stroma
A structured report makes life easier for the surgeon. A typical paragraph might read:
The lowsignal cervical stromal ring is intact on sagittal T2, measuring 4mm in thickness. No focal disruption or parametrial fat infiltration is observed. DWI shows a 1.5cm hyperintense lesion confined to the endocervical canal, without ADC reduction beyond the lesion.
Clinical DecisionMaking
From image to treatment
When the MRI shows an intact stromal ring, many clinicians feel comfortable recommending a fertilitypreserving conization or simple hysterectomy for earlystage disease. Once the ring is broken, the usual recommendation shifts toward radical hysterectomy or chemoradiation, because the tumour has likely entered surrounding tissues.
Reallife scenario
Consider a 28yearold who dreams of having children. Her MRI shows a 1cm lesion confined to the canal, with a perfectly smooth stromal ring. The multidisciplinary team opts for a coldknife conization, preserving fertility. Six months later, repeat MRI confirms no residual disease. Thats the power of accurate stromal assessment.
For patients and clinicians weighing conservative surgery against more aggressive options, understanding longterm outcomes is essential; resources on prostate cancer outlook can offer perspective on how staging influences prognosis across genitourinary cancers and help frame conversations about expectations and followup.
Monitoring response
After chemoradiation, MRI is repeated at 3 and 6month intervals. Youll look for a reestablished dark ring (or at least lack of new disruptions) and a drop in DWI signal. Persistent bright areas could indicate residual tumour and prompt further workup.
When to suspect recurrence
Any new focal loss of the stromal line, especially if paired with a rising serum SCCAg, warrants urgent imaging. Clinicians often use a redflag checklist: new pain, bleeding, or palpable mass plus MRI findings = early referral.
Key Takeaways
- The cervical stroma appears as a thin, lowsignal T2 ring; its continuity is the hallmark of a tumourfree cervix.
- Tumour invasion shows as disruption of that ring, often with spiculated extensions into parametrial fat.
- Highresolution T2, DWI, and early DCE are the three pillars of a reliable cervicalstroma MRI protocol.
- Accurate staging guides whether a patient can have a conservative surgery or needs a more aggressive approach.
- Always pair MRI findings with clinical context; consider PET/CT or ultrasound when the picture is ambiguous.
Weve covered a lot, but the most important message is simple: a clear view of the cervical stroma on MRI can turn uncertainty into confidencefor both the doctor and the patient. If anything in this guide sparked a question or youve lived through a similar imaging story, share it in the comments. Your experience could help someone else navigate the same road.
FAQs
What does cervical stroma look like on MRI?
The cervical stroma appears as a thin, dark (low-signal) ring around the bright endocervical canal on T2-weighted MRI.
Why is the cervical stroma important in cancer staging?
The integrity of the cervical stroma on MRI helps determine if cancer has spread beyond the cervix, directly impacting treatment choices.
How does tumor invasion affect the cervical stroma on MRI?
Tumor invasion disrupts the smooth, dark stromal ring, often causing irregularities, bulges, or breaks visible on MRI.
What MRI sequences are best for evaluating cervical stroma?
High-resolution T2-weighted, DWI, and dynamic contrast-enhanced MRI are essential for assessing cervical stroma.
Can cervical stroma MRI findings change treatment plans?
Yes, an intact stromal ring may allow fertility-sparing surgery, while disruption often leads to more aggressive treatment.