When considering treatments for various cancers, including prostate cancer, understanding the impact of different treatments on life expectancy is crucial. For men undergoing prostate removal, also known as radical prostatectomy, there is a significant survival benefit. The
10-year survival rate for patients after prostate removal is notably high, with studies indicating it can be as high as 91%[2]. This procedure is often recommended for men with localized or intermediate-risk prostate cancer.When evaluating the outcomes of prostate removal, it's essential to consider the broader context of
prostate cancer outlook. This includes understanding the disease's progression and the various treatment options available, such as surgery, radiation, and hormone therapy like
anti-androgens for prostate cancer. For those interested in understanding how life continues after prostate surgery, the ability to lead a normal life is well-documented. While there are side effects, such as erectile dysfunction and incontinence, these can often be managed over time[5]. Further information on living with prostate cancer and managing its effects can be found in discussions about
survival without prostate and
early prostate cancer treatment options.Here are some key points about prostate cancer and its treatment:-
Prostate Removal Life Expectancy: Prostate removal surgery typically does not shorten life expectancy, with most patients experiencing a high survival rate[2][5].-
Survival Without Prostate: After surgery, many men lead active lives, managing side effects as needed[5].-
Early Prostate Cancer: For early-stage disease, surgery is often an effective treatment option, but
early prostate cancer management may involve watchful waiting or other treatments as well[6].
FAQs
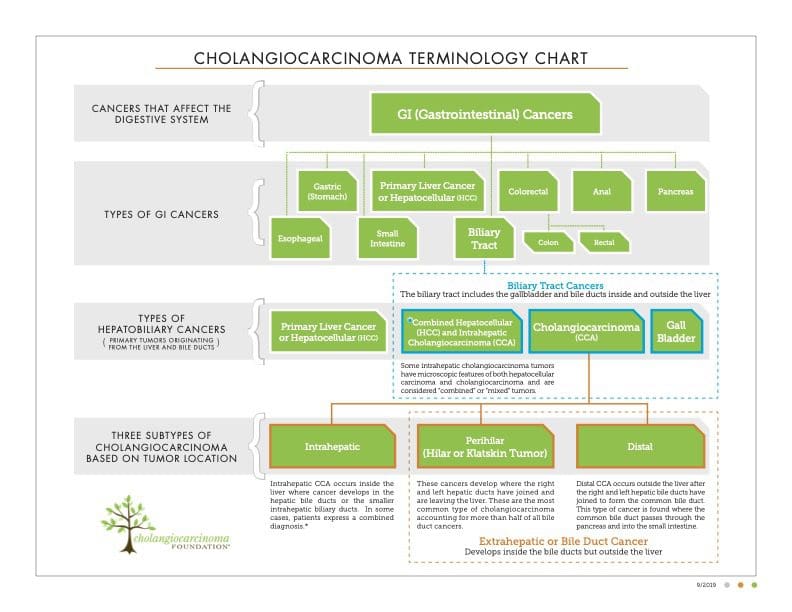
What are the first‑line treatments for cholangiocarcinoma?
The standard first‑line regimen is a combination of gemcitabine and cisplatin chemotherapy. For early‑stage disease, surgery (partial or extended hepatectomy) is preferred, often followed by adjuvant chemotherapy or chemoradiation.
How is operability determined for bile duct cancer?
Operability depends on tumor stage, location, involvement of major blood vessels, and the patient’s liver reserve (future liver remnant >30 %). High‑resolution imaging (MRI/MRCP) and liver function tests help decide if a curative resection is feasible.
When should I consider targeted therapy for cholangiocarcinoma?
If molecular testing shows an FGFR2 fusion or an IDH1 mutation, FDA‑approved targeted agents (pemigatinib for FGFR2‑rearranged, ivosidenib for IDH1‑mutated disease) can be added after or instead of standard chemotherapy.
What role do clinical trials play in cholangiocarcinoma care?
Clinical trials provide access to emerging treatments such as immunotherapy‑chemo combos, novel kinase inhibitors, and personalized vaccine approaches. Enrollment is often recommended when standard options are exhausted or when a trial matches a specific molecular profile.
How can palliative care improve quality of life for advanced cholangiocarcinoma?
Palliative care focuses on symptom relief—bile duct stenting to resolve jaundice, pain management, nutritional support, and psychosocial counseling. These interventions help maintain comfort, independence, and overall wellbeing.