Imagine youve just beat cancer, only to hear another scary wordAML. Its a punch you didnt expect, and it can feel like the ground has shifted under your feet. The truth is, therapyinduced acute myeloid leukemia (tAML) is a rare but real sequel to certain cancer treatments. It can appear months or even years after the original therapy, and knowing what to expect can make the difference between feeling lost and feeling empowered.
In this guide Ill walk you through the essentials: what tAML is, why it happens, the signs to watch for, your prognosis, and the treatment options that exist today. Ill share realworld stories, break down the science in plain language, and give you practical steps you can take right now. Lets dive in together.
What Is tAML?
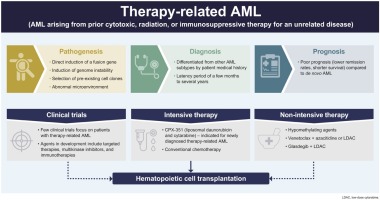
Therapyinduced AML, often called tAML, is a type of acute myeloid leukemia that develops after exposure to certain chemotherapy drugs (like alkylating agents or topoisomeraseII inhibitors) or radiation therapy. Whiledenovo AML arises without a known prior trigger, tAML has a clear link to the treatment that once saved a life.
Key Differences from DeNovo AML
- Latency period: usually 27 years after the original therapy.
- Genetics: more often shows complex cytogenetics and TP53 mutations.
- Prognosis: generally poorer, but outcomes improve with modern targeted therapies.
How Common Is It?
tAML accounts for roughly 10% of all AML cases worldwide. That sounds small, but when you consider the millions of people undergoing chemotherapy each year, the absolute number is not negligible. Recent epidemiologic studies show a gradual rise in reported cases, partly because survivors live longer and were better at detecting secondary leukemias.
Whos at Risk?
Therapies That Raise the Risk
Not all cancer treatments carry the same danger. The biggest culprits are:
- Alkylating agents (e.g., cyclophosphamide, melphalan)
- TopoisomeraseII inhibitors (e.g., etoposide, doxorubicin)
- Highdose radiation, especially to the pelvis or abdomen
Patient Factors
Age, genetic predisposition (like inherited TP53 mutations), and the cumulative dose of the offending drug all play a role. Adults who survived solidtumor cancers such as breast or lymphoma are the largest group, but children can develop tAML toooften after treatment for acute lymphoblastic leukemia (ALL) or solid tumors.
Spotting the Early Signs
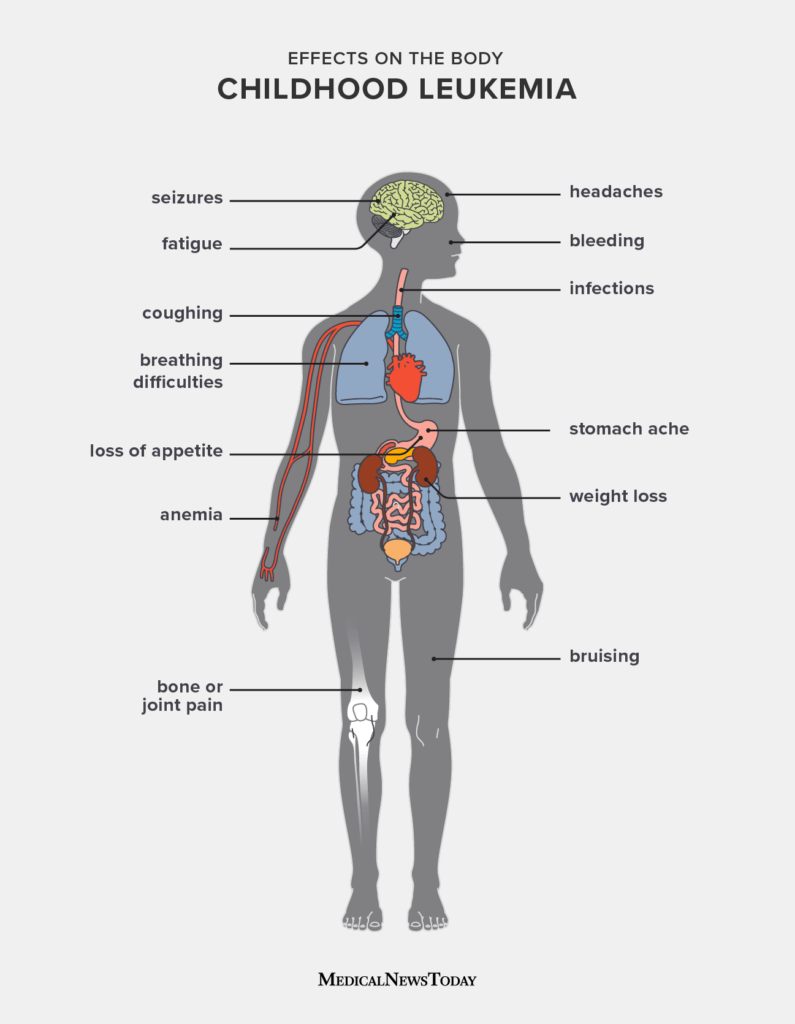
Acute myeloid leukemia can progress rapidly, so catching it early matters. Common red flags include:
- New or worsening fatigue
- Unexplained bruising or bleeding gums
- Frequent infections
- Persistent fever without a clear source
- Unexplained weight loss
If you notice any of these symptoms, especially after a history of chemotherapy or radiation, reach out to your oncologist promptly. A simple complete blood count (CBC) can reveal abnormal blast cells that signal leukemia. In some cases, the journey may intersect with concerns such as leukemia pregnancy treatment for those who are or may become pregnant during or after treatment.
Understanding the Prognosis
Prognosis in therapyrelated AML is a nuanced topic. Historically, median overall survival hovered around 612 months, largely because of adverse cytogenetics. However, recent advances have shifted the landscape.
Key Prognostic Factors
- Age: patients under 60 tend to fare better.
- Cytogenetics: complex karyotype or TP53 mutations portend a poorer outlook.
- Performance status: how well youre able to tolerate intensive therapy.
When you pull all these pieces together, the tAML life expectancy can vary widelyfrom less than a year in highrisk cases to over three years for those with favorable genetics who receive a transplant. Prognosis may be different in younger women, particularly when considering unique situations like AML pregnancy treatment, requiring a specialized multidisciplinary team.
The Genetics Behind tAML
TherapyRelated AML Cytogenetics
Most tAML cases feature abnormal chromosomes. The classic patterns are deletions of 5q and 7q, often accompanied by a complex karyotype (three or more chromosomal abnormalities). These changes are a direct fingerprint of DNA damage caused by the previous therapy.
Common Mutations
In addition to chromosomal alterations, certain gene mutations show up repeatedly:
- TP53: the guardian of the genomemutated in roughly 3040% of tAML.
- RUNX1, ASXL1, NRAS, KRAS: contribute to uncontrolled cell growth.
- FLT3ITD: present in a minority but offers a target for specific inhibitors.
Understanding these mutations isnt just academic; they guide treatment choices, especially when targeted agents are on the table. Genetic testing may sometimes be considered, comparable to colon cancer genetic testing when determining risk or guiding therapy for other cancers.
Pathology and Diagnosis
Diagnosing tAML follows the same criteria as denovo AML, with a few extra notes for the therapyrelated label. According to the WHO 2022 classification, you need:
- 20% myeloid blasts in bone marrow or peripheral blood, or a specific genetic abnormality.
- Evidence of prior exposure to leukemogenic therapy.
On a practical level, a bonemarrow biopsy reveals the blast percentage, while flow cytometry shows the characteristic surface markers (CD34, CD13, CD33, HLADR). For coding and insurance purposes, the ICD10 code for therapyrelated AML is C92.0.
Treatment Options Today
Even though tAML carries a heavier prognosis, modern treatment offers hope. The goal is clear: achieve remission, lengthen survival, and maintain quality of life.
Standard Chemotherapy
The backbone remains the 7+3 regimenseven days of continuous cytarabine infusion plus three days of an anthracycline (like daunorubicin). This approach works for many patients, but those with complex cytogenetics often need something extra.
Targeted Therapies
If your leukemia harbors a FLT3ITD mutation, a FLT3 inhibitor (e.g., midostaurin) can be added to the chemotherapy backbone. Venetoclax, a BCL2 inhibitor, combined with hypomethylating agents (azacitidine or decitabine), has shown promising results especially in older or unfit patients.
StemCell Transplant
Allogeneic hematopoietic stemcell transplantation (alloHSCT) offers the best chance for longterm remission, but its only an option for those with adequate performance status and a suitable donor. Survival after transplant for tAML is lower than for denovo AML, yet many patients still enjoy several years of diseasefree life.
Supportive Care
Because the marrow is fragile, proactive infection prophylaxis, blood product support, and psychosocial counseling are essential. A good oncology team will coordinate these elements seamlessly.
Special Populations
Children
Therapyrelated AML in children is rare (about12% of pediatric AML). When it occurs, its often linked to prior ALL treatment involving anthracyclines and cranial radiation. These cases frequently show KMT2A rearrangements, which can guide specific trial enrollment.
Elderly Patients
Older adults typically have more comorbidities, making intensive chemotherapy risky. For them, lowintensity regimens (like venetoclax+azacitidine) have become the standard of care, balancing efficacy with tolerability.
Balancing Benefits and Risks
Its natural to feel tornyour original therapy saved you from one cancer, but now a new threat looms. Clinicians address this by weighing the absolute risk of tAML (often less than 5% for many regimens) against the proven benefit of the initial treatment. Doseadjustments, using lessleukemogenic agents when possible, and regular monitoring can reduce risk without compromising cure rates.
For survivors, staying informed is the most empowering step. Schedule routine CBCs, discuss any new symptoms promptly, and ask your oncologist about the specific lateeffects monitoring plan for your treatment history.
Quick Reference Tools
TherapyRelated AML at a Glance
| Trigger Therapy | Typical Latency | Common Cytogenetics | Median OS (months) | FirstLine Treatment |
|---|---|---|---|---|
| Alkylating agents (cyclophosphamide) | 37years | 5/7, complex karyotype | 812 | 7+3venetoclax |
| Topoisomerase II inhibitors (etoposide) | 13years | 11q23/MLL rearrangements | 1014 | 7+3FLT3 inhibitor (if mutated) |
| Highdose radiation | 25years | TP53 mutation, complex | 610 | Lowintensity hypomethylating agents venetoclax |
Survivor Checklist
- Annual CBC (or more often if advised).
- Report unexplained bruising, fatigue, fevers immediately.
- Ask your doctor about genetic testing for TP53 or other mutations.
- Consider joining a survivorship support group for emotional backing.
- Keep a written record of all prior therapies and dosesthis helps future physicians assess risk.
RealWorld Stories
Case 1: A 58YearOld BreastCancer Survivor
Maria completed adjuvant cyclophosphamide and radiation five years ago. She began feeling unusually weak and bruised. A CBC revealed 25% blasts. Bonemarrow testing showed a complex karyotype with TP53 loss. She underwent the 7+3 regimen followed by an alloHSCT from a matched sibling. Today, three years posttransplant, shes in complete remission and is an active advocate for survivorship awareness.
Case 2: A 9YearOld with Prior ALL
Little Ethan received a regimen that included highdose anthracyclines and cranial radiation at age three. At age nine, routine labs showed rising blasts. Genetic profiling identified a KMT2AMLLT3 fusion typical of tAML in children. He enrolled in a clinical trial exploring a novel menin inhibitor, achieving a second remission. His family stresses the importance of early detection and staying engaged with the medical team.
Putting It All Together
Therapyinduced AML is undeniably serious, but knowledge equips you to act decisively. By recognizing risk factors, staying vigilant for symptoms, understanding the genetic landscape, and exploring modern treatment paths, you can navigate this challenge with confidence.
Remember, the risk of tAML is relatively low compared to the lifesaving benefit of the original therapy. Still, being proactiveregular blood work, open conversations with your oncology team, and perhaps consulting a hematology specialistcan catch early changes before they snowball.
Conclusion
Therapyinduced AML may feel like an unexpected twist in an already tough journey, but youre not alone. The medical community continues to refine therapies, and patients are benefitting from targeted drugs, transplantation advances, and robust survivorship programs. If you or a loved one face this diagnosis, lean on your care team, seek reputable information, and consider joining support networks. Your experience, questions, and voice mattershare them, stay informed, and keep moving forward.
Whats been your experience with posttreatment monitoring? Have you found a particular resource helpful? Drop a comment below, and lets keep the conversation going.
FAQs
What types of cancer therapy are most likely to cause therapy‑induced AML?
Alkylating agents (e.g., cyclophosphamide, melphalan), topoisomerase II inhibitors (e.g., etoposide, doxorubicin) and high‑dose radiation are the primary culprits. The risk rises with higher cumulative doses and certain genetic predispositions.
What early symptoms should prompt me to get checked for t‑AML?
Watch for new fatigue, easy bruising or bleeding, frequent infections, unexplained fevers, and unexplained weight loss. A simple blood count can detect abnormal blast cells early.
How does the prognosis of therapy‑induced AML differ from de‑novo AML?
t‑AML usually has a poorer outlook because it often carries complex cytogenetics (e.g., deletions of 5q/7q) and TP53 mutations. Median overall survival ranges from 6‑12 months in high‑risk cases to over 3 years when favorable genetics and transplant are possible.
Are there targeted treatments available for t‑AML?
Yes. If the leukemia has a FLT3‑ITD mutation, a FLT3 inhibitor (such as midostaurin) can be added to chemotherapy. Venetoclax combined with hypomethylating agents (azacitidine or decitabine) is effective, especially for older or unfit patients.
What follow‑up care should cancer survivors have to monitor for t‑AML?
Regular CBCs (often annually or more often if advised), prompt reporting of any new bruising or fatigue, and discussing genetic testing for TP53 or other mutations with your oncologist are key steps in survivorship monitoring.