Hey thereif youve just heard the words cns leukemia, chances are a swirl of worry and questions has taken over. You might be wondering what it actually means, how it shows up, and whether theres hope on the horizon. Im here to walk you through the essentials, cut through the jargon, and give you the clear, friendly answers you need right now.
What Is CNS Leukemia?
In plain English, CNS leukemia is when leukemia cellsthose rogue bloodforming cellsfind their way into your central nervous system, which includes the brain and spinal cord. Its not a completely separate disease; its a complication of the more familiar blood cancers, but it demands its own attention because the brain is a very delicate place.
Understanding CNS1, CNS2, and CNS3
Doctors use a threetier system to describe how much leukemia has infiltrated the cerebrospinal fluid (CSF). Think of it like traffic lights:
| Stage | CSF Blast Count | Key Features | Typical Prognosis |
|---|---|---|---|
| CNS1 | No blasts, 5WBC/L | Lowest risk, often no neurological symptoms | Best survival outlook |
| CNS2 | No blasts, >5WBC/L | Elevated white cells, may need prophylaxis | Intermediate outlook |
| CNS3 | 5WBC/L with blasts | Highest disease burden, needs intensive therapy | More guarded survival |
These categoriesCNS1, CNS2, CNS3guide how aggressive the treatment should be. A pediatric oncologist will often tell families that being at CNS3 is like getting a red light; we have to act fast and strong.
Who Gets It?
While any leukemia patient can develop CNS involvement, its more common in certain subtypes (like acute lymphoblastic leukemia) and in children. Adults, especially those over 60, tend to have a tougher time because their bodies handle intensive therapy differently.
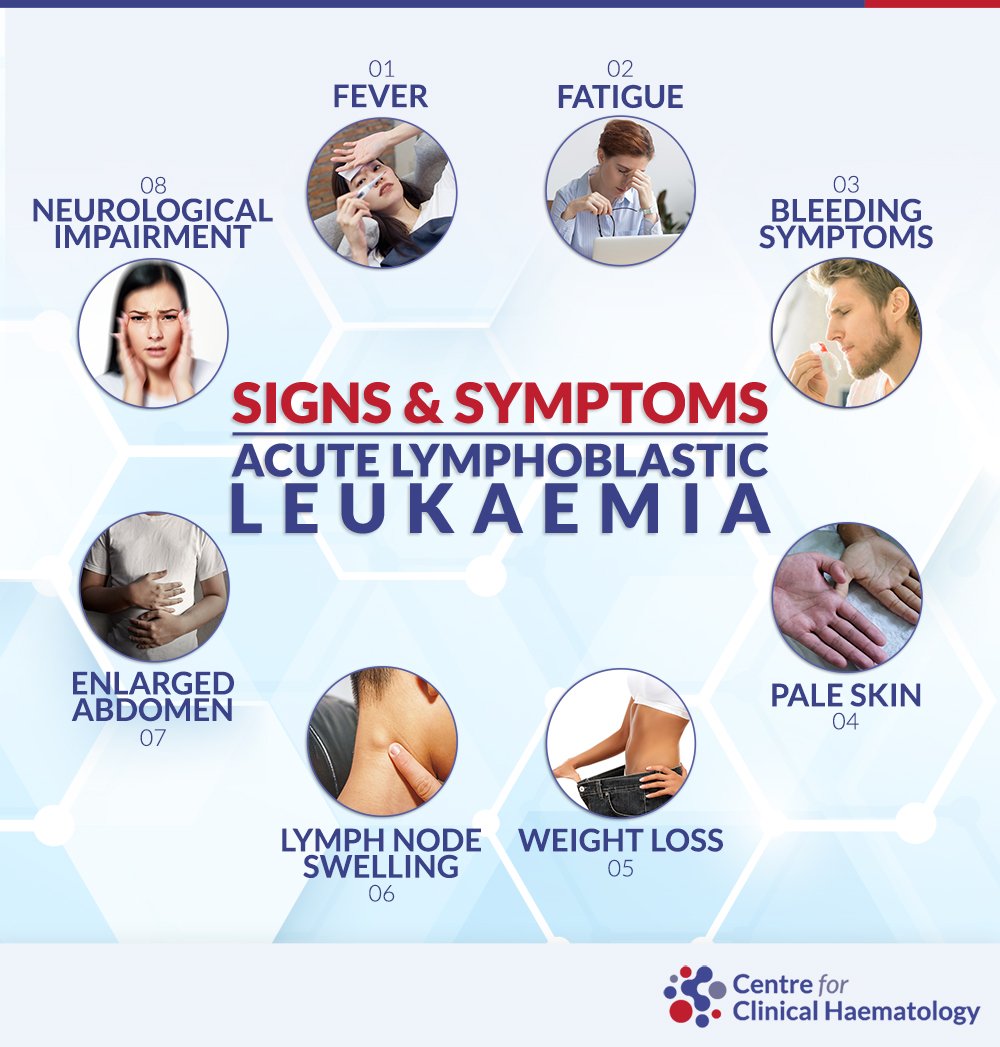
Key CNS Leukemia Symptoms
Spotting the warning signs early can make a world of difference. Heres a quick checklist that you can keep on hand or share with a loved one.
Neurological Red Flags
- Persistent, worsening headache that doesnt improve with typical pain relievers.
- Visual disturbancesblurry vision, double vision, or sudden loss of sight.
- Sudden weakness or numbness in one arm or leg.
- Seizures, especially if youve never had them before.
- Difficulty with balance or walking, feeling offkilter.
Systemic Clues That Point to CNS Spread
- Fever or chills without an obvious infection.
- Unexplained fatigue that feels deeper than ordinary tiredness.
- Blood test showing a sharp rise in white blood cells.
Childrens Specific Signs
Kids dont always say I have a headache. Instead, watch for irritability, vomiting (especially in the morning), or a bulging fontanellethose soft spots on a baby's skull that can swell when pressure builds up inside the brain.
RealWorld Example
Take Mark, a 45yearold accountant who thought his bad migraine was just stress. After three weeks of worsening pain and a sudden episode of blurred vision, a lumbar puncture revealed CNS3 leukemia. The early red flagspersistent headache and visual changewere the clues that led to a lifesaving diagnosis.
Diagnosing CNS Leukemia
Getting a solid diagnosis is like gathering pieces of a puzzle. You need a combination of lab work, imaging, and sometimes a bit of detective work.
Lumbar Puncture & CSF Analysis
The gold standard is a lumbar puncturean outpatient procedure where a needle is slipped into the lower back to collect cerebrospinal fluid. The fluid is then examined for blasts (leukemia cells) using cytology and flow cytometry. According to , CSF flow cytometry catches about 90% of CNS involvement, far better than traditional cytology alone.
Imaging: CNS Leukemia Radiology
Magnetic Resonance Imaging (MRI) is the goto scan because it shows subtle meningeal (membrane) enhancementthose faint, glowing lines that signal leukemia cells crawling along the brains coverings. CT scans can be used in emergencies, but they miss many early changes.
Molecular & Cytogenetic Testing
Beyond just counting blasts, labs now look for genetic mutations like NPM1, FLT3, or the Philadelphia chromosome. These markers can influence both prognosis and the choice of targeted therapy.
Diagnostic Checklist (Quick Reference)
| Step | What to Do | Why It Matters |
|---|---|---|
| 1 | Order complete blood count (CBC) | Baseline for systemic disease |
| 2 | Perform lumbar puncture with CSF flow cytometry | Detects CNS1/2/3 status |
| 3 | Get brain MRI with contrast | Shows meningeal involvement |
| 4 | Run molecular panel (e.g., FLT3) | Guides targeted drugs |
| 5 | Consult multidisciplinary team | Ensures balanced treatment plan |
Survival Outlook Overview
Its natural to ask, What are my chances? The answer depends on many moving partsage, disease stage, genetic profile, and how well the treatment works.
Overall CNS Leukemia Survival Rate
For adults with CNS3 disease, fiveyear overall survival (OS) hovers around 3040%. If youre caught at CNS1, that number climbs above 70% when modern protocols are used. Children fare better, with a fiveyear survival rate often exceeding 80% thanks to aggressive prophylaxis and tailored therapy.
Factors That Shift the Numbers
- Age: Younger patients usually tolerate highdose chemotherapy better.
- CNS Stage: As the table shows, CNS3 carries the toughest prognosis.
- Genetics: Certain mutations (e.g., FLT3ITD) may lower survival, but targeted inhibitors can offset that risk.
- Transplant Eligibility: Those who can undergo an allogeneic stemcell transplant often see improved longterm outcomes.
Leukemia in Brain Survival Rate Compared
When you compare leukemia in brain to CNS1/2/3 categories, the numbers line up: earlystage (CNS1) patients have survival rates similar to general ALL survival, while CNS3 aligns with the lower end of the spectrum. This underscores why precise staging matters.
Treatment Options Overview
Now, lets talk about what actually helps. Treatment for CNS leukemia is a blend of systemic chemotherapy, intrathecal (directly into the CSF) drugs, and sometimes radiation. The goal is to eradicate leukemia cells everywhere while keeping side effects manageable.
Standard Chemotherapy Backbone
Most patients receive highdose methotrexate and cytarabine, both of which cross the bloodbrain barrier. These drugs are given in cycles, interspersed with intrathecal injections (usually methotrexate + cytarabine) to mop up any lingering cells in the CSF.
Targeted & Immunotherapy Breakthroughs
In the past few years, CD19CAR Tcell therapy has shown promiseeven for CNS diseasebecause the engineered T cells can traffic into the brain. BTK inhibitors, like ibrutinib, also have modest CNS penetration and are being explored in clinical trials.
Radiotherapy (CNS Leukemia Radiology)
Radiation is like a doubleedged sword. It can quickly shrink meningeal disease, but it may also cause longterm cognitive changes, hormonal imbalances, or secondary cancers. Doctors usually reserve it for refractory cases or when urgent control is needed.
StemCell Transplant
If youre a good candidate, an allogeneic transplant can offer a resetreplacing your diseased marrow with healthy donor cells. The transplant graftversusleukemia effect can clear residual CNS disease, but the procedure carries risks like graftversushost disease.
Balancing Benefits & Risks
Every treatment has upside and downside. Intensive chemo may increase remission chances but also raise infection risk. Radiation can control disease fast but may affect memory later. Thats why shared decisionmakingtalking openly with your oncologist about your values and lifestylematters.
Decision Flowchart (Quick Guide)
| Step | Consideration | Typical Action |
|---|---|---|
| 1 | CNS1 status? | Systemic chemo + intrathecal prophylaxis |
| 2 | CNS2 or highrisk features? | Highdose methotrexate + intensified intrathecal schedule |
| 3 | CNS3 disease? | Combine systemic + intrathecal + consider radiation |
| 4 | Eligible for transplant? | Proceed to allogeneic stemcell transplant after remission |
| 5 | Targetable mutations? | Add targeted agents (e.g., BTK inhibitor) |
Relapse Prevention Tips
Even after you beat the disease, staying vigilant is key. Heres how you can help keep the leukemia at bay.
Intrathecal Prophylaxis Schedules
Most protocols call for an intrathecal injection every 23weeks during the consolidation phase, then tapering to every 23months for up to two years. Your nurse can walk you through the exact timetable.
Surveillance Imaging & CSF Checks
After treatment, doctors usually order a brain MRI and a repeat lumbar puncture at 3month intervals for the first year, then every 6months. Keeping these appointments is crucialearly detection of a tiny resurgence can be a gamechanger.
Lifestyle & Support
- Stay hydratedlots of water helps clear the CSF.
- Monitor for infections; a fever should prompt a call to the clinic.
- Engage in gentle exercise (walking, yoga) to boost immunity.
- Seek neurocognitive assessments if you notice memory fog; early rehab can mitigate longterm effects.
Printable Patient Checklist
Feel free to copy this list for your next doctor visit:
- Ask about the current CNS stage (CNS1/2/3).
- Confirm the intrathecal schedule and any upcoming lumbar punctures.
- Request the latest MRI dates and ask what findings to look for.
- Discuss any new neurological symptoms, even if they seem minor.
- Review sideeffect management plans (e.g., nausea, neuropathy).
Takeaway & Next Steps
Weve covered a lot: what CNS leukemia is, the redflag symptoms, how doctors nail the diagnosis, what the survival numbers look like, and the toolbox of treatmentsfrom chemotherapy to CART cells. The key takeaway is that early recognition and a wellcoordinated treatment plan dramatically improve outcomes, especially when youre aware of your CNS stage (CNS1,2,3) and the specific therapies that fit.
If you or someone you love is navigating this journey, the best next step is to have a candid conversation with a hematologyoncology specialist. Bring your questions, ask for a clear explanation of the CNS stage, and discuss both the potential benefits and the possible risks of each treatment option. Remember, youre not alonesupport groups, patientnavigator services, and even simple checkin calls with friends can make a huge difference.
Whats your experience with CNS leukemia? Have you found a particular resource or coping tip especially helpful? Share your story in the comments below; wed love to hear from you. And if anything in this article sparked a new question, dont hesitate to askyou deserve clear, compassionate answers. For related information on treatment considerations during pregnancy, see AML pregnancy treatment.
FAQs
What is CNS leukemia?
CNS leukemia occurs when leukemia cells spread to the central nervous system, including the brain and spinal cord, making it a serious complication of blood cancers like acute lymphoblastic leukemia. It is not a separate disease but a form of advanced disease involvement[5].
What are the main symptoms of CNS leukemia?
Symptoms can include headaches, nausea, vomiting, visual disturbances (blurry or double vision), seizures, unexplained weakness or numbness, balance problems, and changes in mental alertness. In children, watch for irritability, vomiting, or a bulging fontanelle (soft spot on a baby’s head)[5][9].
How is CNS leukemia diagnosed?
Diagnosis involves a lumbar puncture (spinal tap) to examine cerebrospinal fluid for leukemia cells, MRI scans of the brain and spine, blood tests, and sometimes molecular testing for specific genetic mutations. CSF analysis is key for staging as CNS-1, CNS-2, or CNS-3[5].
What treatments are available for CNS leukemia?
Treatment typically combines high-dose chemotherapy (often methotrexate and cytarabine), intrathecal chemotherapy (directly into the spinal fluid), and sometimes radiation or stem cell transplant. Targeted therapies and CAR-T cell therapy are emerging options for certain cases[2][3].
What is the outlook for someone with CNS leukemia?
Prognosis depends on the stage at diagnosis, age, genetics, and response to treatment. Early-stage (CNS-1) disease has a better outlook, while CNS-3 carries a more guarded prognosis. Children generally have higher survival rates than adults due to more aggressive treatment protocols[5].