Finding a lump in your chest can feel like a punch to the gut. Is it something harmless you can ignore, or does it signal a more serious issue? In most cases the answer lies in the specific chest tumor type youre dealing with. Knowing whether a growth is benign or malignant, where it started, and how it behaves is the first step toward the right tests, the proper treatment, and a realistic outlook on life expectancy. Below, Ill walk you through the most common chest tumors, how they differ between men and women, the symptoms that truly matter, and what options are available if you need care.
Primary vs. Secondary
Chest tumors fall into two broad camps. Primary tumors start right in the chest wallbone, cartilage, or soft tissue. Secondary tumors, on the other hand, are metastases that have traveled from another part of the body, like the breast or lung. This distinction matters because it determines the treatment pathway: primary tumors often require surgery or localized radiation, whereas secondary tumors usually need systemic therapy that targets the original cancer site.
Common Primary Tumors
When doctors hear chest tumor, they usually think of a handful of sarcomas that arise in the rib cage or surrounding structures. Heres a quick snapshot of the most frequently encountered types:
| Tumor Type | Origin Tissue | Typical Age | Benign / Malignant |
|---|---|---|---|
| Chondrosarcoma | Cartilage | 3070years | Malignant (most common) |
| Ewing Sarcoma | Bone/soft tissue | <20years | Malignant |
| Osteosarcoma | Bone | 2040years | Malignant |
| Rhabdomyosarcoma | Skeletal muscle | Childrenadolescents | Malignant |
| Plasmacytoma | Plasma cells | 5070years | Malignant (often precedes myeloma) |
| Malignant Fibrous Histiocytoma | Soft tissue | 5070years | Malignant |
| Benign Osteochondroma | Cartilagebone | Teens20s | Benign |
These figures line up with the data compiled by StatPearls, a trusted medical reference that many clinicians turn to for quick, evidencebased overviews.
Rare Benign Tumors
Not every chest wall growth is a cancerous beast. Benign tumorssuch as lipomas, hemangiomas, and fibrous dysplasiacan still cause discomfort, cosmetic concerns, or anxiety. Even though they dont spread, doctors usually recommend imaging and sometimes removal, especially if they grow or press on nerves.
Symptoms Overview
Chest tumor symptoms can be subtle, and they often overlap with everyday aches. The key is to notice patterns that dont resolve with rest or overthecounter pain relievers.
General RedFlag Signs (All Genders)
- Persistent, painless lump that doesnt change size over weeks.
- Unexplained chest pain that worsens with deep breathing or coughing.
- Visible swelling, skin dimpling, or a tight feeling across the chest wall.
FemaleSpecific Clues
Women sometimes notice a mass that seems to blend with the breast tissue or appears near the ribs. shows a gallery of female chest wall tumors pictures that illustrate how these lesions can mimic breast lumps, making imaging essential for a correct diagnosis.
MaleSpecific Clues
Guys often report a firm, nontender nodule right in the middle of the chestwhat many refer to as a painless lump in middle of chest male. Because it can be mistaken for costochondritis, a quick Xray or CT scan is the best way to rule out a tumor in chest male scenario. For men considering prostate health along with cancer concerns, information about prostate removal life expectancy can provide important context on treatment outcomes.
Quick What Could It Be? Checklist
Before you book an appointment, run through this short list ( means yes, I have this):
- Lump feels hard and fixed, not soft or mobile.
- No recent injury to the area.
- Growth faster than 1cm per month.
- Accompanied by night sweats, unexplained weight loss, or persistent coughing.
If you check any of those boxes, its time to see a doctorpreferably one who specializes in thoracic oncology.
Diagnostic Pathway
FirstLine Imaging
Most doctors start with a plain Xray to spot obvious bone involvement. An ultrasound can be helpful for superficial softtissue masses, especially when trying to distinguish a cyst from a solid tumor.
Advanced Imaging
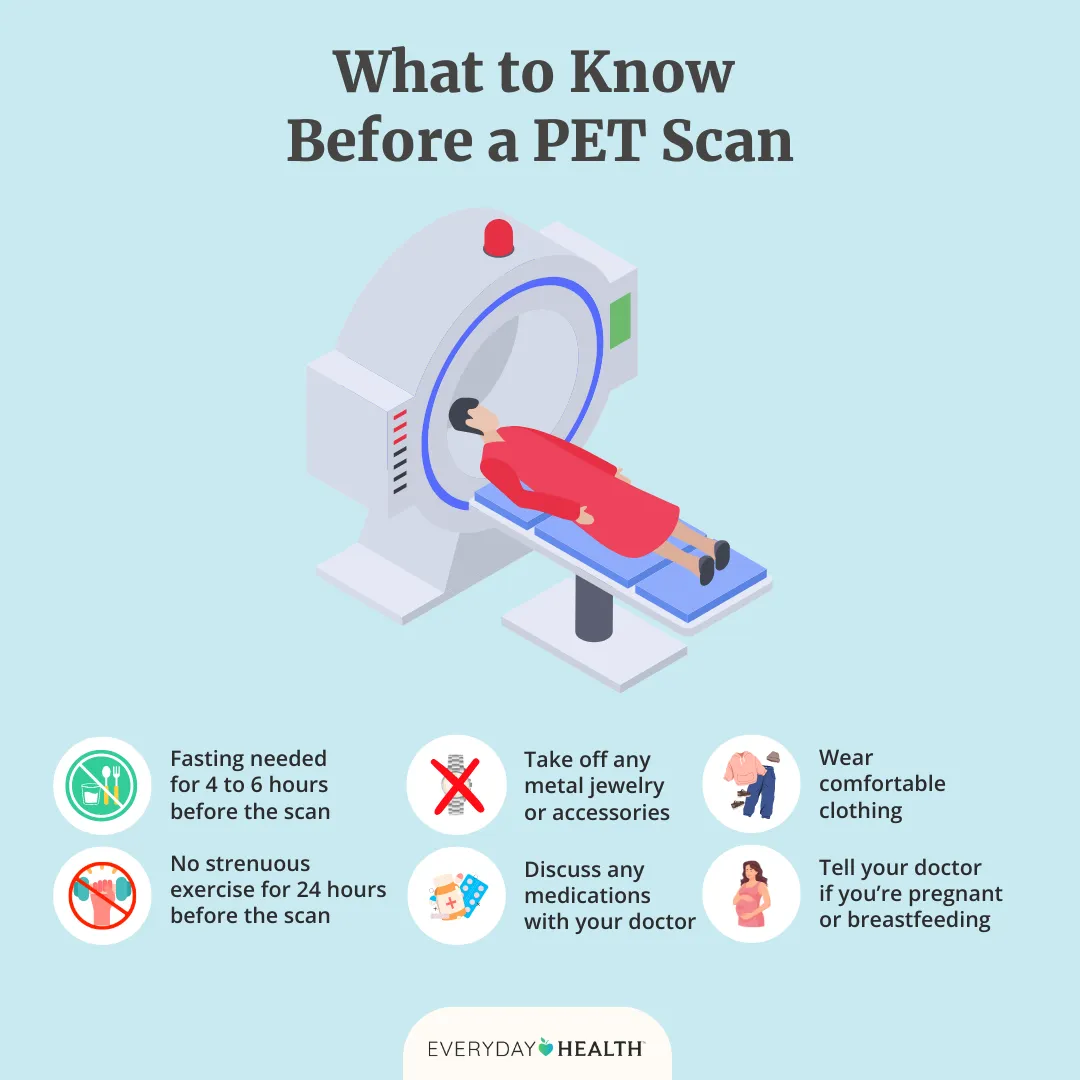
A CT scan provides a detailed view of bone erosion, rib involvement, and the exact size of the lesion. MRI shines when we need to map softtissue extension, neurovascular involvement, or the relationship to the lung and heart. In select cases, a PET scan helps gauge metabolic activityuseful for staging and for later followup.
Biopsy & Histopathology
The definitive answer comes from tissue. Coreneedle biopsy is the most common, but a surgeon may perform an incisional biopsy if the mass is large or located in a tricky spot. Pathologists look for specific markersS100 for chondrosarcoma, CD99 for Ewing sarcoma, Desmin for rhabdomyosarcomato pin down the exact tumor type.
Dr. Alex Smith, a thoracic surgical oncologist at Mount Sinai, often says, A clear histologic diagnosis changes the treatment algorithm dramatically, highlighting why a biopsy is not just a formality but a turning point in care ().
Treatment Options
Surgery The Gold Standard
When the tumor is resectable, surgery aims for clean marginsusually at least a 2cm rim of healthy tissue. Resection may require reconstructive techniques, such as synthetic mesh or muscle flaps, to restore chest wall stability and protect the lungs.
Radiation Therapy
Radiation can be used after surgery if margins are close, or as a primary option when the tumor cannot be removed safely. Modern techniques like IMRT (intensitymodulated radiation therapy) focus the dose while sparing the heart and lungs.
Systemic Therapies
Highgrade sarcomas often respond to multiagent chemotherapydoxorubicin combined with ifosfamide is a common backbone. Certain tumors, such as plasmacytoma, may benefit from targeted agents like proteasome inhibitors, especially if they evolve into multiple myeloma.
Emerging & Clinical Trials
Immunotherapy is an exciting frontier. Early trials with checkpoint inhibitors are showing promise for a subset of chest wall sarcomas. If youre open to experimental approaches, ClinicalTrials.gov lists ongoing studies you can explore with your oncologist.
DecisionTree Flowchart (Visual Aid)
Imagine a simple flowchart:
- Notice symptom get Xray/US.
- Advanced imaging (CT/MRI) suspicious mass?
- Biopsy identify tumor type.
- Multidisciplinary review surgery radiation chemo.
- Followup imaging schedule.
This roadmap helps keep the process transparent and reduces the feeling of being in the dark.
Prognosis and Life
Factors That Influence Survival
Age, tumor grade, size, location, and whether you can achieve clean surgical margins all play a role. For example, a small, lowgrade chondrosarcoma in a 45yearold who undergoes complete resection often enjoys a long, healthy life. In contrast, a large, highgrade Ewing sarcoma that has already spread may need aggressive multimodal therapy and carries a higher recurrence risk.
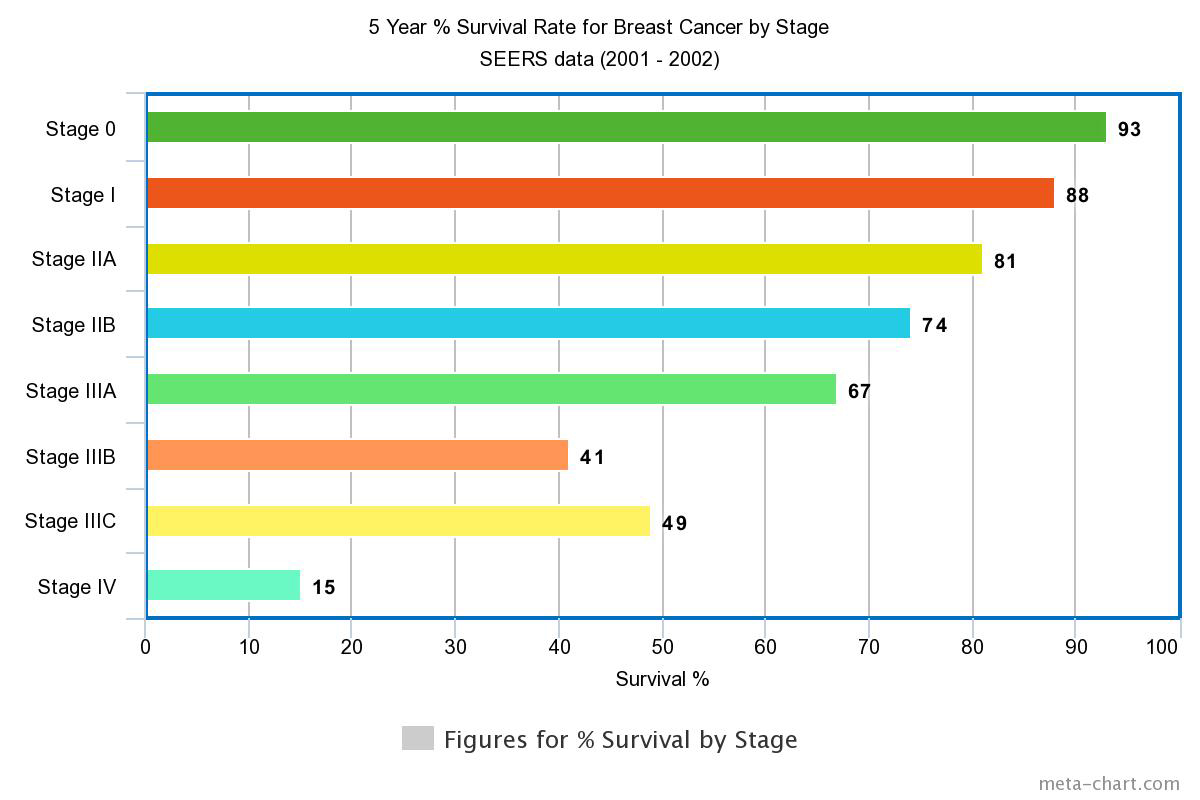
Chest Wall Cancer Life Expectancy by Type
| Tumor Type | 5Year Survival | Typical Recurrence |
|---|---|---|
| Chondrosarcoma | 7085% | Lowtomoderate |
| Ewing Sarcoma | 5570% (localized) | High (needs multimodal therapy) |
| Osteosarcoma | 4560% | Moderate |
| Rhabdomyosarcoma | 6080% (children) | Variable |
| Plasmacytoma | 8090% (isolated) | High risk of progression to myeloma |
These numbers are drawn from the European Society of Thoracic Surgeons patientinformation sheets ().
Quality of Life Considerations
Beyond numbers, living with a chest tumor impacts breathing, posture, and sometimes selfimage. Postoperative pain management, pulmonary rehabilitation, and support groups can make a huge difference. If you or a loved one is navigating this journey, dont underestimate the power of a good physiotherapist or a community forum where people share their daytoday victories. Similarly, patients dealing with prostate cancer often explore information about prostate cancer outlook to understand their long-term health trajectory.
Personal Story (Experience Insight)
Take Maya, a 42yearold teacher who discovered a small, painless lump on her left rib cage during a routine selfexam. Imaging revealed a lowgrade chondrosarcoma. After a widelocal excision and mesh reconstruction, she returned to the classroom within three months. Her biggest takeaway? Ask questions earlydont wait for the lump to grow up. The quicker you get a diagnosis, the more options you have.
Resources & Further Reading
If you want to dive deeper, these sources are reliable and easy to understand:
- StatPearls Chest Wall Tumors (comprehensive medical overview)
- (patientfriendly explanations and images)
- (expert clinical pathways)
- (prognosis tables and survivorship tips)
- (quick symptom guide)
Most of these sites let you download printable cheatsheets, so you can keep a handy reference when youre talking to your healthcare team.
Conclusion
Chest tumor types span a wide spectrumfrom harmless osteochondromas you can monitor, to aggressive sarcomas that demand swift, coordinated care. Understanding the specific tumor, the symptoms that matter (and how they differ between men and women), and the most accurate diagnostic steps empowers you to ask the right questions and collaborate effectively with your doctors. With the right information, you can explore all treatment avenuesincluding clinical trialswhile keeping a realistic view of prognosis and quality of life.
If youve felt that knot in your chest or have concerns about a recent diagnosis, dont wait. Schedule an imaging appointment, request a referral to a thoracic oncology specialist, and bring this guide with you. Knowledge is not just powerits peace of mind.
FAQs
What are the most common primary chest tumor types?
The most frequently seen primary chest tumors include chondrosarcoma, Ewing sarcoma, osteosarcoma, rhabdomyosarcoma, plasmacytoma, malignant fibrous histiocytoma, and benign osteochondroma.
How can I tell if a lump in my chest is a tumor?
Key warning signs are a hard, painless, fixed lump that doesn’t change with movement, rapid growth, unexplained chest pain, night sweats, weight loss, or persistent coughing. Any of these should prompt imaging and medical evaluation.
What imaging tests are used to diagnose chest tumor types?
Initial evaluation usually starts with a chest X‑ray or ultrasound. CT scans give detailed bone and size information, MRI maps soft‑tissue involvement, and PET scans assess metabolic activity for staging.
When is surgery the preferred treatment for chest tumor types?
Surgery is the gold standard when the tumor is resectable with clean margins. It often involves removing the mass plus a 2‑cm rim of healthy tissue and may require chest‑wall reconstruction with mesh or muscle flaps.
What is the typical prognosis for chest tumor types?
Prognosis varies by tumor type, grade, size, and margin status. For example, low‑grade chondrosarcoma has a 5‑year survival of 70‑85 %, while high‑grade Ewing sarcoma (localized) ranges from 55‑70 %.