If youve discovered that several close relatives have cancers linked to Lynch syndrome, or youve faced a diagnosis of colorectal or endometrial cancer yourself, you might be asking: Should I get tested? The answer is a clear yesbut only if you understand the why, who, what, and how. Below, Ill walk you through everything you need to know, from eligibility rules to costs, so you can make an informed, confident decision.
Why Testing Matters
What are the benefits of confirming a Lynchsyndrome diagnosis?
Pinpointing a pathogenic variant in the mismatchrepair (MMR) genes (MLH1, MSH2, MSH6, PMS2, EPCAM) does more than label a condition. It opens the door to earlier, more frequent colonoscopies, targeted surveillance for extracolonic cancers, and even preventive surgeries. Most importantly, it empowers you to share accurate risk information with family members, potentially saving lives. For people considering broader cancer risk planning, resources on colon cancer genetic testing can help clarify which genes and panels are most relevant.
What are the potential risks or downsides?
Receiving genetic information can stir up anxiety, especially when the results are uncertain. Moreover, concerns about insurance discrimination still linger, even though the Genetic Information Nondiscrimination Act (GINA) offers federal protection. A balanced viewthat benefits often outweigh the emotional and financial challengeshelps keep the decision grounded.
Quick riskmanagement checklist
- Schedule pretest genetic counseling.
- Confirm the labs accreditation (CAP, CLIA).
- Review your insurers policy on genetic testing.
- Identify a support network (family, patient groups).
Who Should Test
Familyhistory thresholds 3 relatives rule
The National Comprehensive Cancer Network (NCCN) recommends testing when a first or seconddegree relative trio meets the classic Lynchsyndrome pedigree: at least three relatives with colorectal, endometrial, ovarian, stomach, or smallbowel cancer, especially when diagnoses occur before age50.
Personalhistory triggers
A personal diagnosis of colorectal cancer, endometrial cancer, or any MMRdeficient tumor (shown by microsatellite instability or loss of MMR protein expression) automatically meets testing criteria. Even a single earlyonset colorectal cancer can be enough.
Tumortesting flags
When pathology reports show MSIhigh status or loss of MLH1, MSH2, MSH6, or PMS2 on immunohistochemistry, NCCNs advise reflex germline testing.
Table: Tumorscreening results Recommended genetic test
| Tumor Finding | Recommended Action |
|---|---|
| MSIhigh | Proceed to germline panel testing |
| Loss of MLH1/PMS2 | Test for BRAF V600E or MLH1 promoter methylation; if negative, do germline test |
| Loss of MSH2/MSH6 | Direct germline testing for MSH2/MSH6 |
Current Guideline Landscape
NCCNs 20242025 recommendations
The NCCN advises that anyone meeting the familial or personal criteria should be offered a multigene panel test on a blood sample at any age, though many clinicians start discussions by age2025.
ACG clinical guideline highlights
The American College of Gastroenterology (ACG) mirrors NCCN but adds that for individuals with a known pathogenic variant, colonoscopic surveillance should begin at age2025 or 25years before the youngest case in the familywhichever comes first.
CDCs publichealth stance
According to the , nationwide screening rates for Lynch syndrome remain low, emphasizing the need for cliniciandriven education and clear testing pathways.
Types of Genetic Tests
Blooddraw laboratory panels
Standard panels analyze the five core MMR genes plus EPCAM. They are the gold standard, offering high sensitivity and the ability to detect large deletions.
Athome saliva kits
Several FDAcleared kits let you spit into a tube and mail it back. Accuracy rivals blood tests for most variants, but a genetics professional must still interpret the results before any clinical action.
Wholeexome or targeted nextgeneration sequencing
These broader panels can uncover rare or novel variants but come with higher costs and a greater chance of ambiguous findings (variants of uncertain significance, or VUS).
Comparison table: Blood vs. Saliva vs. NGS
| Method | Cost (USD) | Turnaround | Insurance Coverage |
|---|---|---|---|
| Blood panel | $500$1,200 | 23 weeks | Often covered with documentation |
| Saliva kit | $300$800 | 34 weeks | Variable; many pay outofpocket |
| NGS (wholeexome) | $1,500$3,000 | 46 weeks | Rarely covered |
How Testing Is Performed
Pretest genetic counseling
Before any sample is taken, a certified genetics counselor walks you through potential outcomes, privacy safeguards, and next steps. This session satisfies NCCNs requirement for informed consent and reduces posttest anxiety.
Sample collection
Whether youre in a clinic for a venipuncture or receiving a mailed saliva kit, the collection process takes less than 10 minutes. Kits come with prepaid return envelopes, making the logistics painless.
Laboratory analysis & quality controls
Certified labs follow CMS Laboratory Developed Test (LDT) code L34912 for Lynchsyndrome panels, ensuring consistent accuracy across providers.
Timeline infographic (text version)
- Week0: Counseling & sample collection.
- Week12: Lab processing.
- Week3: Results reviewed with counselor.
- Week4: Followup care plan established.
Interpreting Test Results
Positive pathogenic variant
A clear yes means you carry a diseasecausing mutation. Immediate steps include personalized cancerscreening schedules and discussion of riskreducing options.
Variant of Uncertain Significance (VUS)
A VUS is a gray area. It doesnt confirm risk, but it also isnt benign. Your counselor may recommend periodic reevaluation as scientific knowledge evolves.
Negative result
A negative result doesnt always mean youre out of the woodsespecially if a strong family history exists. You may still need surveillance based on pedigree alone.
Case vignette: Janes journey
Jane, 32, tested negative for the known family mutation, yet two cousins were diagnosed with colorectal cancer before 45. Her counselor advised continued colonoscopy every 35years, illustrating that genetics is only part of the risk puzzle.
Surveillance & Management
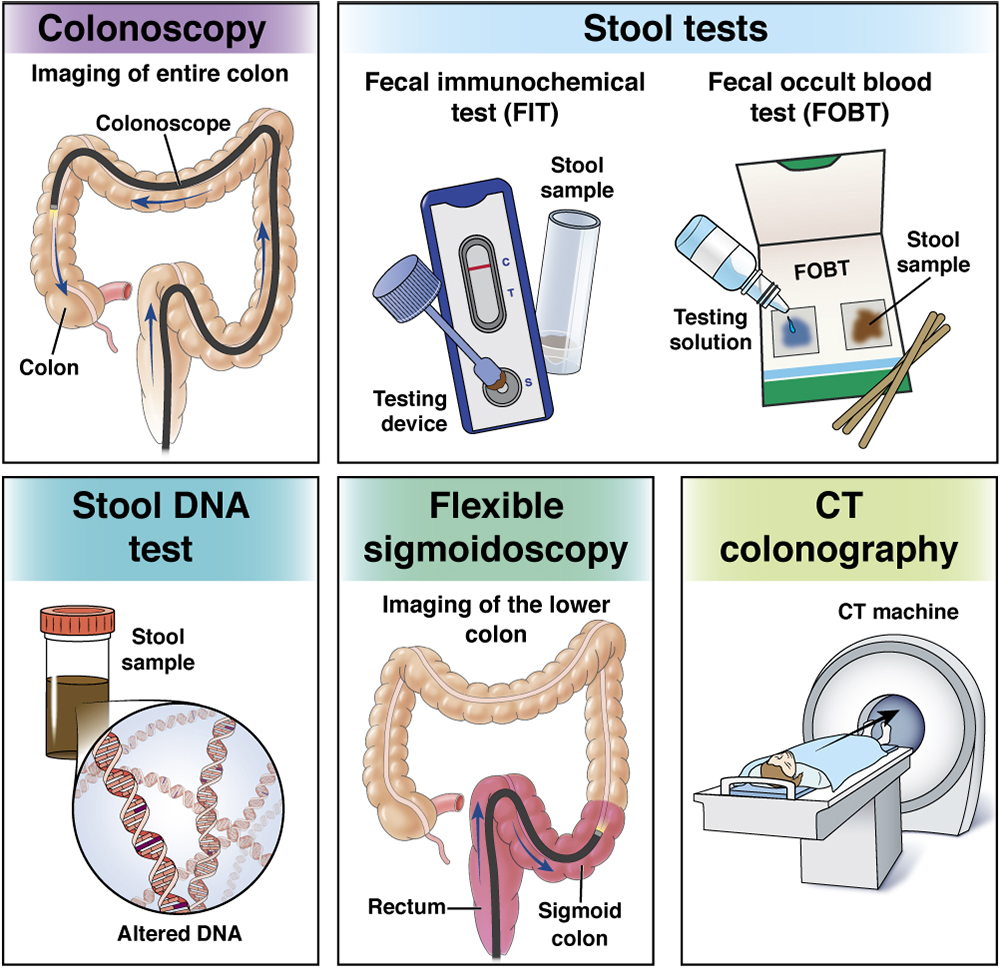
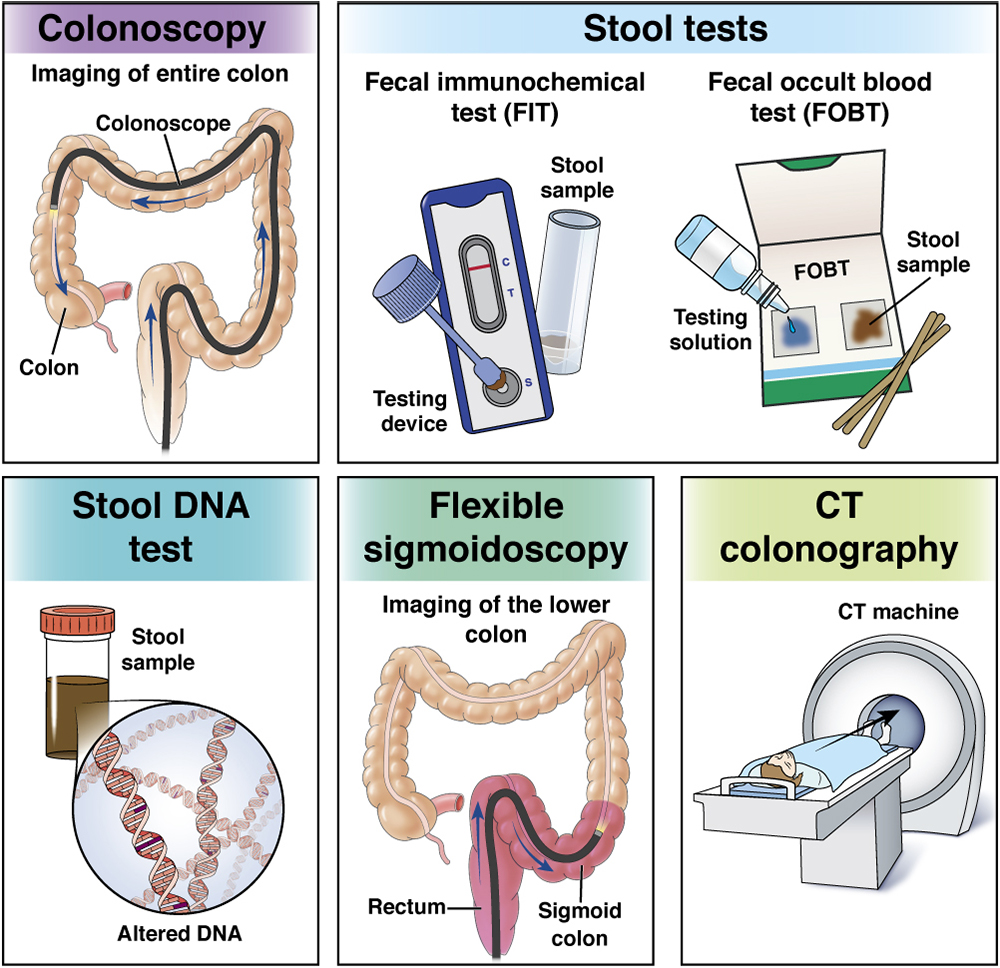
Colonoscopic screening schedule
For carriers, NCCN recommends colonoscopy every 12years beginning at age2025, or 25years before the youngest diagnosis in the family. This aggressive schedule has been shown to reduce colorectal cancer mortality by up to 70%.
Extracolonic cancer screening
Women with a pathogenic variant should consider annual endometrial sampling and transvaginal ultrasound starting at 3035years. Gastric and ovarian screening protocols vary, but many specialists suggest upper endoscopy every 35years for highrisk families.
Riskreducing surgery options
Colectomy (removal of part or all of the colon) and prophylactic hysterectomy with bilateral salpingooophorectomy can dramatically lower cancer risk. Deciding on surgery is deeply personal and usually follows thorough counseling about fertility, quality of life, and recovery.
Decisionmaking checklist
- Assess age and family cancer chronology.
- Discuss reproductive plans.
- Weigh surgical risks versus surveillance fatigue.
- Consider psychological readiness.
Cost & Access
Lynch syndrome testing cost
In 2024, a standard blood panel averages $800$1,200. Saliva kits can be a bit cheaper, ranging $300$800, but insurance coverage often favors the blood draw.
Insurance coverage
Medicare and most private insurers cover testing when NCCN criteria are met (see CMS Laboratory Developed Test code L34912). However, you may need to submit a priorauthorization letter that outlines your family history.
Financial assistance programs
Many academic centers and nonprofit groups offer slidingscale fees or grant assistance. A sample letter to insurers (downloadable from patient advocacy sites) can expedite approvals.
Sample insurerletter excerpt
Dear Medical Director, per NCCN guidelines, my patient meets the criteria for Lynchsyndrome germline testing due to a documented threegeneration history of earlyonset colorectal cancer. I request coverage for a multigene panel (CPT 81211). Thank you for your prompt attention.
RealWorld Experience
Case Study A 32yearold with MSH2 mutation
After a positive test, Alex began colonoscopies every 18months and opted for prophylactic hysterectomy at 35. He reports peace of mind knowing his risk is actively managed.
Patient Quote B I wish Id been tested earlier
Maria, diagnosed with endometrial cancer at 38, reflects that early genetic insight could have prompted earlier colonoscopies for her relatives, potentially catching cancer at a more treatable stage.
Tips from survivors
- Keep a written familyhistory log.
- Bring a trusted friend to counseling sessions.
- Ask providers about telecounseling if travel is a barrier.
Trusted Resources Guide
Official guideline PDFs
Download the latest NCCN and ACG documents directly from their websites for the most uptodate recommendations.
CDC hereditary colorectal cancer portal
A valuable resource for publichealth statistics, educational videos, and screening tools.
Professional societies (ASCO, ACMG)
These groups publish consensus statements on ethical considerations, test interpretation, and insurance advocacy.
How to verify a labs accreditation
- Check for CLIA certification on the labs website.
- Confirm CAP accreditation for quality assurance.
- Look up the labs LDT code (e.g., L34912 for Lynchsyndrome panels).
Conclusion
Understanding the lynch syndrome genetic testing guidelines isnt just an academic exercise; its a lifeline for you and your loved ones. When you meet the familyhistory or personalhistory thresholds, a blood or saliva test can unlock a personalized surveillance plan, inform preventive surgery decisions, and guide family members toward early detection. Yes, the financial and emotional costs can feel heavy, but with pretest counseling, clear insurance pathways, and supportive resources, the benefits usually far outweigh the risks.
Take the first step today: schedule a genetics counseling session, gather your familys cancer history, and ask your doctor about the appropriate test. By acting now, youre not only protecting your healthyoure giving future generations a clearer, safer path.
FAQs
Who should undergo Lynch syndrome genetic testing?
Testing is recommended for individuals with a personal or family history of Lynch-associated cancers, especially if three close relatives have such cancers diagnosed before age 50, or if tumors show microsatellite instability or loss of MMR protein expression.
What genes are tested in Lynch syndrome genetic panels?
Standard testing panels analyze mismatch repair (MMR) genes: MLH1, MSH2, MSH6, PMS2, and EPCAM. Expanded panels may include other cancer risk genes based on personal and family history.
What are the benefits of confirming a Lynch syndrome diagnosis?
It enables tailored cancer surveillance (like earlier colonoscopies), targeted screening for extracolonic cancers, consideration of preventive surgeries, and informing at-risk relatives for early intervention.
How is Lynch syndrome genetic testing performed?
Testing is typically done on a blood sample analyzed in an accredited lab. Saliva-based kits are also available but require professional interpretation. Testing is preceded by genetic counseling to ensure informed consent and understanding.
What does a Variant of Uncertain Significance (VUS) result mean?
A VUS means the test found a genetic variant whose impact is unclear. It does not confirm increased cancer risk but may require periodic reevaluation as scientific knowledge advances.