You're probably here because you (or someone you care about) just heard the words synovial sarcoma and felt a rush of questions. The good news? The most effective treatments are welldefined, and with the right information you can navigate the journey with confidence. Below you'll find a clear, step-by-step walkthrough of current treatment recommendationsfrom the surgery that often cures early disease, to the chemo protocols and emerging drugs that keep stage-4 patients alive longer.
Think of this guide as a friendly chat over coffee: we'll talk about symptoms, pathology, the whole surgical and medical playbook, and how to balance benefits with risks. Grab a notebook, and let's dive in.
What Is Synovial Sarcoma?
Typical Symptoms and Warning Signs
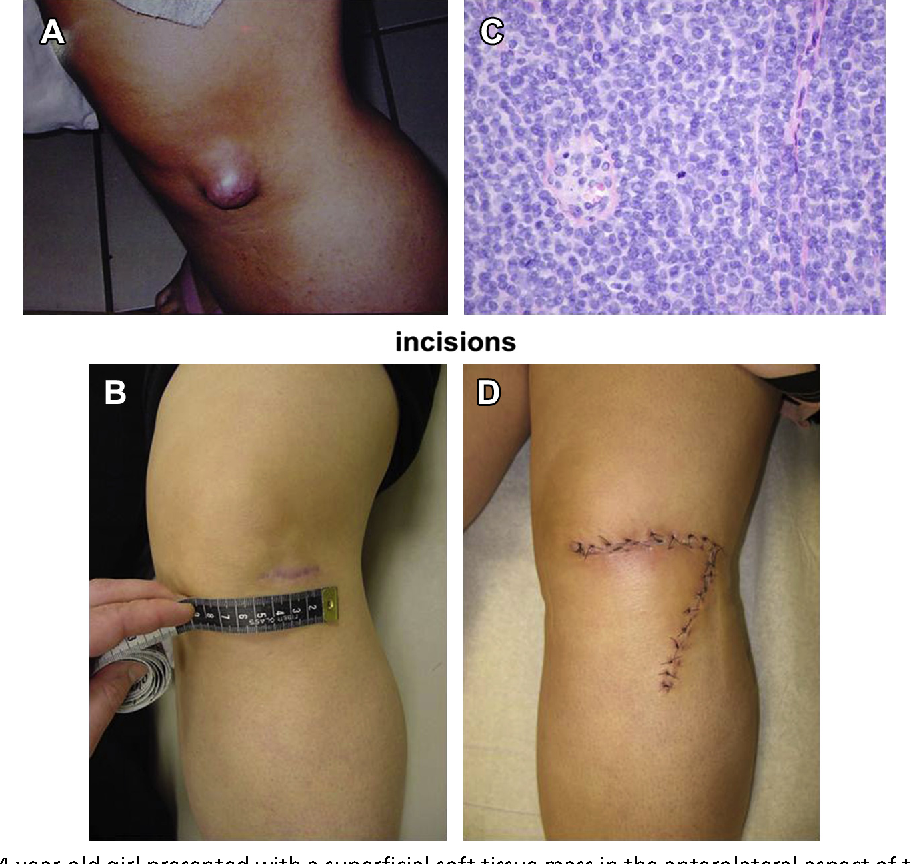
Synovial sarcoma most often masquerades as a harmless lump. Common clues you shouldn't ignore include:
- Persistent, deep-seated pain that worsens at night.
- A firm, mobile mass near a jointespecially the knee, ankle, or shoulder.
- Swelling or reduced range of motion without a clear injury.
If any of these sound familiar, an MRI is usually the next step. Early detection dramatically improves outcomes.
Pathology & Subtypes
Under the microscope, synovial sarcoma can appear in two main flavors:
- Monophasic mostly spindle-shaped cells; slightly easier to treat.
- Biphasic a mix of spindle and epithelial cells; often a tad more aggressive.
Understanding the subtype helps tailor the chemotherapy regimen. For a visual overview, check out early prostate cancer, which includes clear pathology outlines.
Staging Basics Focus on Stage4
Staging follows the AJCC system, where the biggest jump is from localized disease (Stage 13) to stage 4, meaning distant metastasismost often in the lungs. Here's a quick snapshot:
| Stage | Key Features |
|---|---|
| 1 | Small tumor (<5cm), no nodal involvement, no metastasis |
| 23 | Larger size or nodal spread, still no distant metastasis |
| 4 | Distant metastasis (usually lungs) |
Epidemiology & Survival
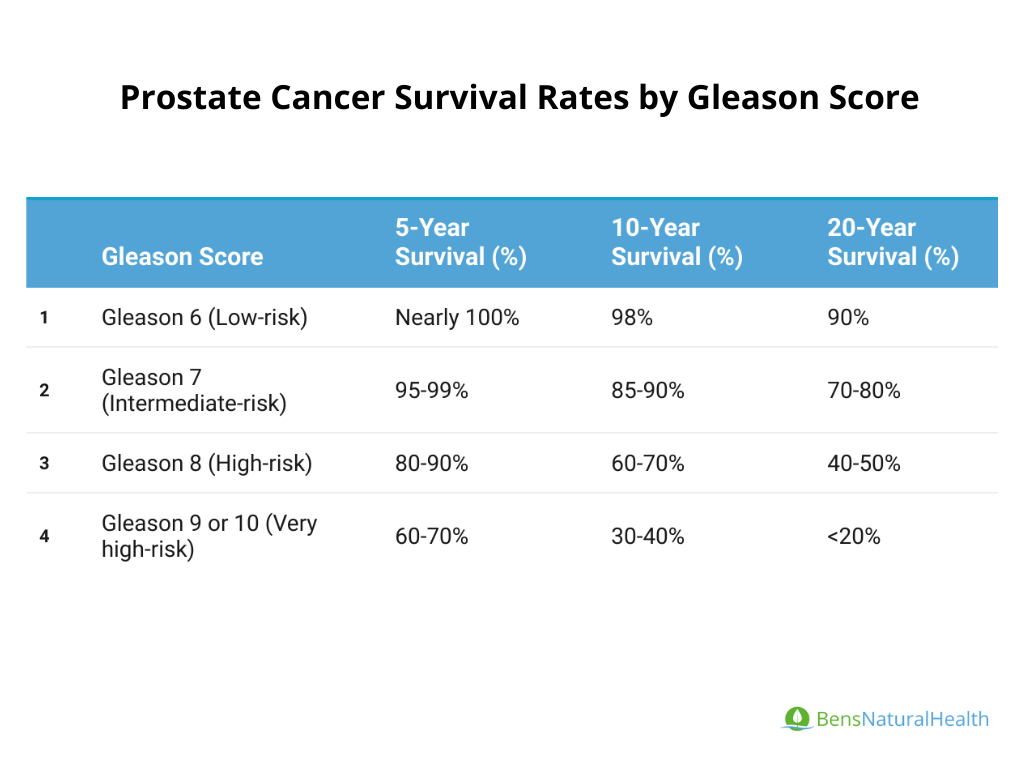
Synovial sarcoma is rareabout 1% of adult soft-tissue sarcomas. Overall 5-year survival hovers around 60%, but once it reaches stage 4, the figure drops to roughly 2030% (see discussion on prostate cancer outlook for a parallel on how stage affects prognosis). These numbers highlight why aggressive, multimodal therapy matters.
Primary Treatment Options
Surgical Management The Cornerstone
When it comes to sarcomas, surgery is the hero. Goal: remove the tumor with a clean margin of healthy tissue (13 cm is the sweet spot). Modern centers aim for limb-sparing resections, preserving function while still achieving oncologic control.
Key steps include:
- Preoperative imaging (MRI + CT) to map the tumor.
- Intraoperative frozen section to confirm clear margins.
- Reconstruction (often with tendon transfers or endoprostheses) if needed.
Amputation is now rare, reserved for cases where the tumor invades critical neurovascular structures.
Radiotherapy When and How
Radiation is the trusty sidekick, especially when margins are close or the tumor is high-grade. Two main strategies exist:
- Preoperative 50 Gy in 25 fractions; it can shrink the tumor and make surgery easier.
- Postoperative 6066 Gy in 3033 fractions; used when margins are positive or uncertain.
Both approaches have comparable local control rates, but preop radiation usually results in fewer long-term fibrosis complications.
Multidisciplinary Care
No single specialist can cover all bases. A typical sarcoma tumor board includes:
- Orthopedic or surgical oncologist
- Medical oncologist
- Radiation oncologist
- Pathologist specialized in soft-tissue tumors
- Physical therapist & psycho-oncology support
This team approach not only optimizes treatment sequencing but also ensures you get the emotional and rehabilitative support you deserve.
Safety & Complications
Every treatment carries risk. Surgical complications can include wound infection, nerve injury, or chronic pain. Radiation may lead to skin changes, edema, or, rarely, secondary malignancies. The key is transparent discussionknowing the odds helps you weigh them against potential cure.
Systemic Therapy Options
Standard Chemotherapy Protocol
If you're facing a high-grade tumor or metastatic disease, chemotherapy steps in. The most widely accepted synovial sarcoma chemotherapy protocol combines:
- Ifosfamide 2 g/m/day for 3 days
- Doxorubicin 75 mg/m as a single infusion
This combo is given every 3 weeks, usually for 46 cycles, with careful monitoring of kidney function and cardiac ejection fraction.
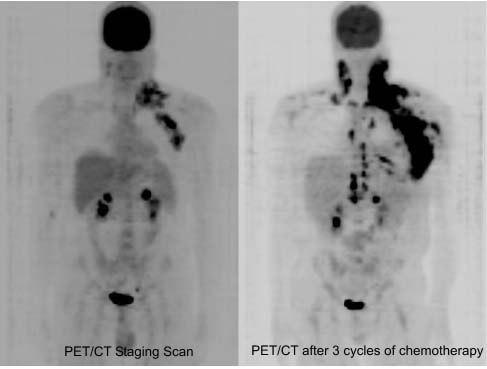
Metastatic (Stage4) Management
When the cancer has spread, the goal shifts to prolonging life and preserving quality. Options include:
- First-line chemo (Ifosfamide + Doxorubicin) offers response rates of 3040%.
- Metastasectomy surgical removal of isolated lung nodules can extend survival for select patients.
- Clinical trials always worth discussing; many trials now focus on targeted agents.
Median overall survival for stage 4 patients receiving modern multimodal therapy hovers around 1824 months, a notable improvement over historic figures.
Targeted Agents & Emerging Therapies
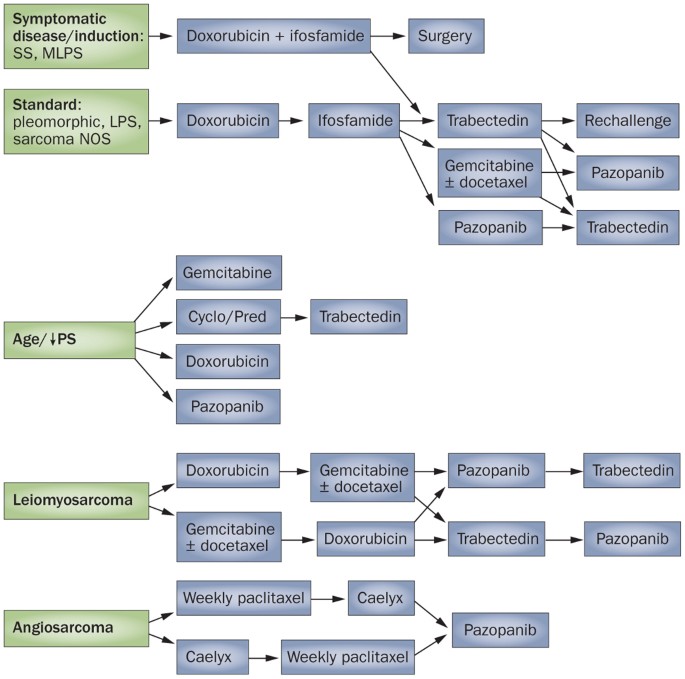
In the past few years, a handful of drugs have entered the sarcoma toolbox:
- Pazopanib an oral VEGFR inhibitor; improves progression-free survival but can cause hypertension and liver enzyme elevations.
- Tazemetostat an EZH2 inhibitor recently FDA-approved for certain sarcomas; early data show modest activity.
- Immunotherapy checkpoint inhibitors (PD-1/PD-L1) are under investigation; results are mixed, but some patients experience durable responses.
When discussing options, ask your oncologist about ongoing trialsaccess to cutting-edge care can make a real difference.
Adjuvant & Neoadjuvant Strategies
Sometimes chemo is given before surgery (neoadjuvant) to shrink the tumor, making a limb-sparing operation possible. Other times, it follows surgery (adjuvant) to mop up microscopic disease. The choice hinges on tumor size, location, and whether margins are clear.
Special Clinical Scenarios
Monophasic Synovial Sarcoma Does Histology Change Management?
Monophasic tumors often respond a touch better to chemotherapy, translating into a slightly higher 5-year survival (about 5% above biphasic). However, surgical principles remain the samewide excision with negative margins.
Stage4 Pathways Decision Tree
Here's a simplified flow:
- Confirm metastasis (usually CT chest).
- Multidisciplinary evaluation.
- Discuss systemic therapy vs. metastasectomy.
- Reassess response; consider clinical trial enrollment.
This roadmap helps keep the conversation focused and avoids unnecessary delays.
Post-Treatment Surveillance
Even after a successful operation, vigilance is key. A typical follow-up schedule looks like:
- MRI of the primary site every 36 months for the first 2 years, then annually.
- Chest CT every 6 months for the first 2 years, then yearly.
- Physical exam and blood work at each visit.
These intervals are backed by both NCCN and UK sarcoma guidelines, aiming to catch recurrences early when they're most treatable.
Pregnancy & Fertility Considerations
If you're a young adult facing a diagnosis, it's natural to worry about future family-building. Discuss fertility preservation (egg or sperm banking) before starting chemo, and ask about the safest timing for pregnancymost experts recommend waiting at least 12 months after completing treatment.
Patient-Centred Decision Making
Balancing Benefits & Risks
Every treatment choice is a tradeoff. Below is a quick matrix to help you weigh options:
| Treatment | Potential Benefit | Common Risks |
|---|---|---|
| Surgery | Potential cure for localized disease | Wound infection, functional loss |
| Radiation | Improved local control | Skin changes, long-term fibrosis |
| Chemo (Ifosfamide + Doxorubicin) | Tumor shrinkage, metastasis control | Kidney toxicity, heart damage |
| Pazopanib | Extended progression-free survival | Hypertension, liver issues |
Shared-Decision Aids
Before your next appointment, print out a short checklist:
- What are my short-term goals? (e.g., preserve limb function)
- What are my long-term goals? (e.g., return to work, family planning)
- What side-effects am I willing to tolerate?
- Do I have questions about clinical trial availability?
Having these bullets ready turns a passive consultation into an active partnership.
Support Networks & Resources
Finding people who get it can make a world of difference. Consider joining:
- Mayo Clinic's patient portal for sarcoma (offers webinars and Q&A sessions).
- The Sarcoma Foundation's support groupsboth online and in-person.
- NCI's Sarcoma Hotline for quick answers.
Financial & Insurance Navigation
High-cost drugs and repeated imaging can strain budgets. Tips to ease the burden:
- Ask your oncology office for a financial counsellorthey can help with preauthorizations.
- Check if your treatment qualifies for clinical trial coverage (many trials cover the drug cost).
- Explore nonprofit assistance programs that subsidize travel for treatment at specialized centers.
Conclusion
Synovial sarcoma may feel like an overwhelming storm, but the treatment landscape is clearer than ever. Surgery remains the cornerstone, often paired with thoughtfully timed radiation. When the disease spreads, a well-chosen chemotherapy protocolaugmented by targeted agents like pazopanib or clinical-trial optionscan prolong life and preserve quality. Understanding your tumor's pathology, stage, and the nuanced balance of benefits versus risks empowers you to make confident, shared decisions with your care team.
Remember, you're not alone on this path. Lean on multidisciplinary experts, connect with supportive communities, and keep the conversation open with your loved ones. If you have questions about any of the guidelines above, reach out to your oncologistknowledge truly is the best medicine.
FAQs
What is the first-line treatment for synovial sarcoma?
The primary treatment for synovial sarcoma is surgical removal of the tumor with clear margins, often combined with radiotherapy to improve local control.
Which chemotherapy drugs are standard for synovial sarcoma?
The standard chemotherapy regimen usually combines ifosfamide and doxorubicin, given every 3 weeks, especially for high-grade or metastatic disease.
How is stage 4 synovial sarcoma managed?
Stage 4, involving distant metastasis (typically lungs), is managed with first-line chemotherapy, possible surgical removal of lung nodules (metastasectomy), and consideration of clinical trials for targeted therapies.
What role do targeted therapies play in synovial sarcoma treatment?
Targeted agents like pazopanib and tazemetostat are emerging treatments that improve progression-free survival and offer options beyond chemotherapy in advanced or metastatic cases.
How often should patients be monitored after synovial sarcoma treatment?
Follow-up typically includes MRI of the primary site every 3-6 months for 2 years and annually thereafter, along with chest CT scans at similar intervals to detect recurrence early.