Quick-Answer Summary
If you or a loved one is being treated for leukemia or lymphoma, the most common CNS relapse symptoms are persistent headache, fever, nausea or vomiting, visual changes, seizures, and newonset weakness or numbness. Spotting any of these signs should prompt an immediate call to the oncology team for a lumbar puncture and CSF analysis. For patients and caregivers wondering about post-treatment quality of life and outlook after procedures that affect the pelvic area, resources on prostate removal life expectancy can help set expectations about recovery and long-term functioning.
What Is a CNS Relapse
Definition & Coding
A CNS (central nervous system) relapse means cancer cells have returned to the brain or spinal cord after a period of remission. In medical records this is often coded under cns relapse icd 10 (e.g., C91.0C96.9 for leukemic involvement).
Expert Insight
According to a 2023 review in , CNS relapse occurs in roughly 57% of acute lymphoblastic leukemia (ALL) patients, with higher rates in those who had highrisk features at diagnosis.
Why Understanding Symptoms Matters
Balancing Benefits & Risks
Detecting symptoms early can dramatically improve survival, while delayed recognition often leads to more aggressive disease and complex treatment. Think of it like catching a tiny leak before it floods the whole house.
RealWorld Impact
Emma, a 12yearold with ALL, thought her pounding headache was just stress from school. A few days later, a sudden seizure forced an urgent MRI that revealed CNS relapse. Because the team acted fast, she could start intrathecal chemotherapy within 24hours, and her prognosis improved significantly.
Core CNS Relapse Symptoms
Headache & Pressure
Persistent, worsening headacheespecially if its worse at night or wakes you upis the most frequently reported sign, showing up in about 48% of symptomatic patients.
Symptom Checklist
| Symptom | Typical Frequency | Key Clues |
|---|---|---|
| Headache | 48% | Nighttime worsening, not relieved by usual meds |
| Nausea/Vomiting | 35% | Often paired with visual changes |
| Fever | 30% | Unexplained, not linked to infection |
| Seizures | 12% | Newonset, no prior history |
| Weakness/Numbness | 8% | Localized, may affect one side |
Fever & Systemic Signs
A lowgrade fever that stubbornly refuses to go away can be a red flag, especially if it appears during maintenance therapy when infection is less likely.
Clinical Tip
Distinguish leukemic fever from infection by checking whitecell differentials and performing a quick blood culture; persistent fevers with normal cultures often point toward CNS involvement.
Neurologic Deficits
Sudden weakness, tingling, or facial droop may signal that cancer cells are pressing on specific nerve pathways. Seizures, though less common, are a clear alarm bell.
Illustrative Example
John, a 38yearold undergoing postremission therapy, noticed his left hand felt clumsy and then developed a brief seizure. Imaging confirmed isolated CNS relapsewhat could have been missed if not for his attentiveness.
Visual Changes & Optic Swelling
Blurry vision, double vision, or loss of peripheral sight often accompany optic nerve involvement. If you notice any sudden eye changes, think of them as a vision alarm.
Quick SelfCheck
Do you have any of these? Persistent headache, fever, nausea, vision blur, weakness, or seizures? If yes, call your medical team now.
Less Common Signs
Symptoms like abdominal distension, night sweats, or unexplained fatigue can also appear, especially in isolated cns relapse in all cases where the disease hides outside the usual spots.
How Symptoms Differ by Disease Context
ALL vs. AML vs. Lymphoma
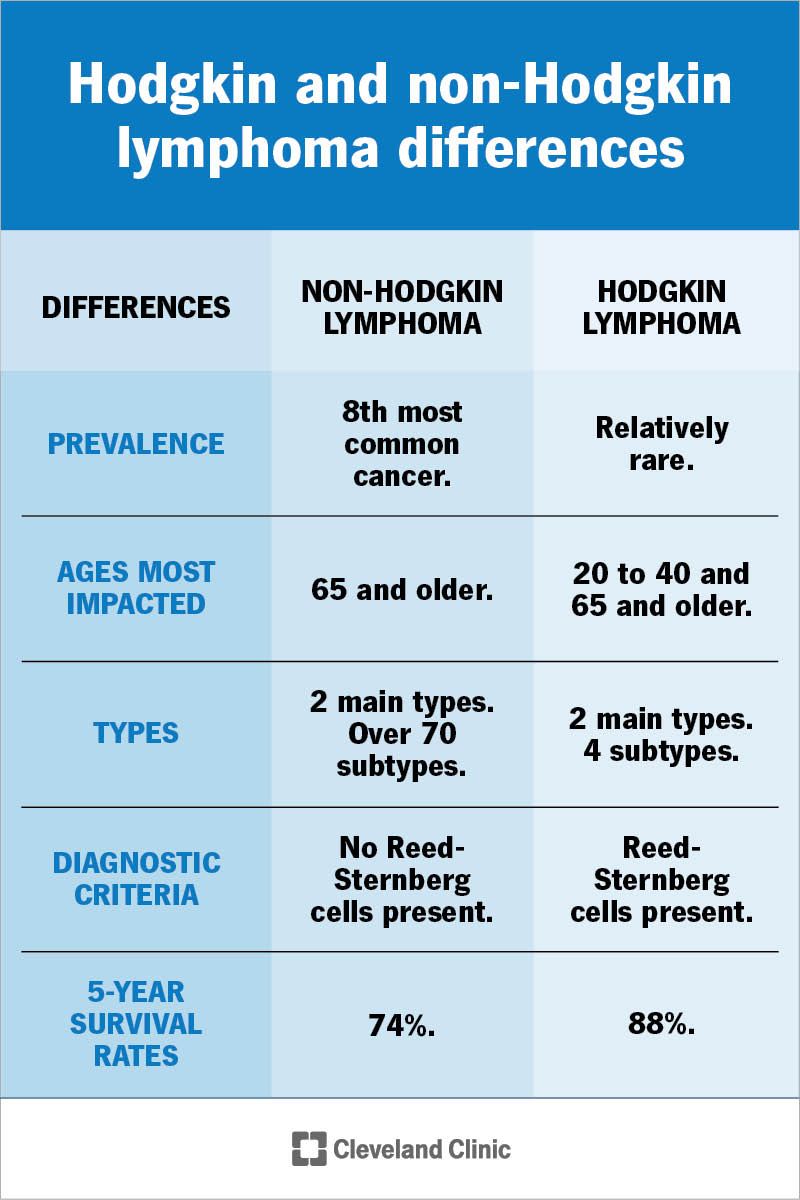
While ALL patients often present with headache and fever, AMLrelated CNS involvement may lean more toward nausea and visual disturbances. Secondary CNS lymphoma typically brings confusion, seizures, and cranialnerve palsies.
Comparison Table
| Condition | Most Frequent Symptom | Unique Signs |
|---|---|---|
| ALL (isolated) | Headache, fever | Abdominal distension |
| AML (CNS) | Nausea, vision changes | Mood swings, balance loss |
| CNS lymphoma | Confusion, seizures | Cranialnerve palsy |
Diagnostic Pathway When Symptoms Appear
FirstLine Evaluation
Start with a thorough physical and neurologic exam, basic blood work, and a review of recent imaging. Nothing replaces a good bedside assessment.
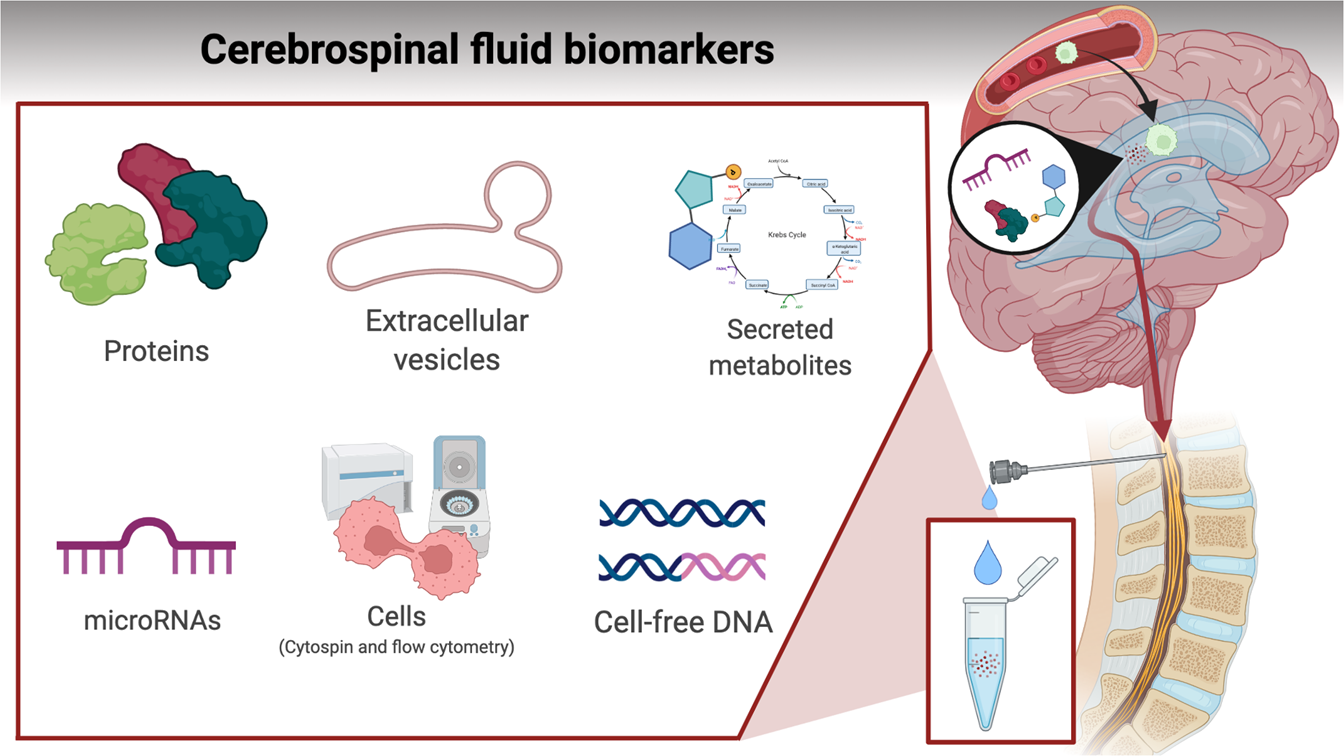
CSF Analysis Steps
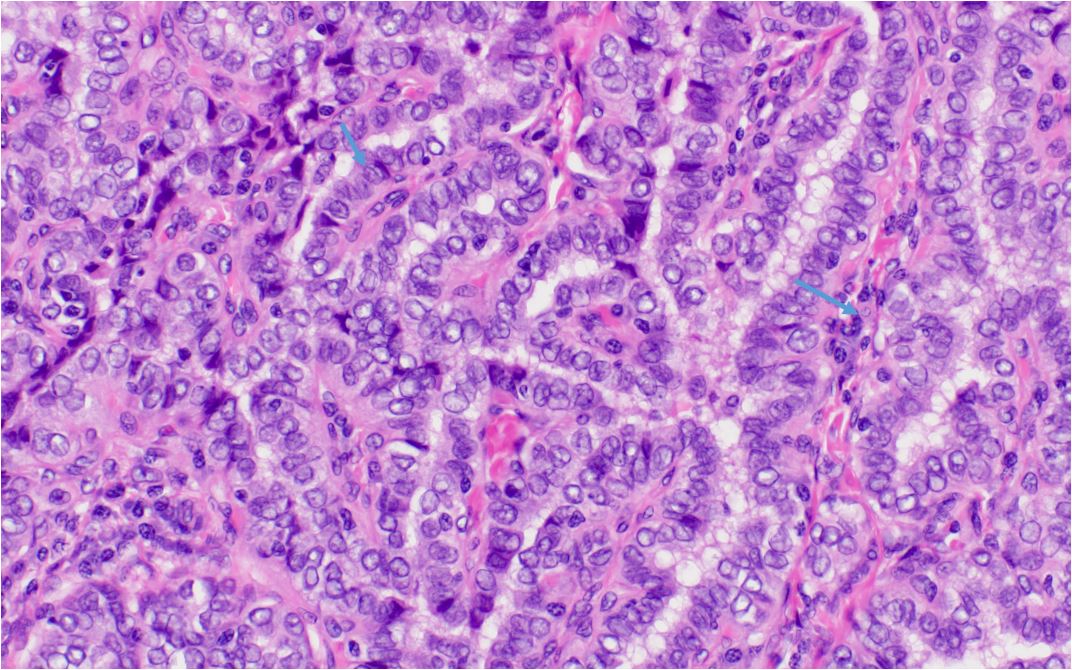
When suspicion is high, a lumbar puncture is performed. The cerebrospinal fluid (CSF) is examined for cell count, cytology, and flow cytometry to detect malignant blasts. A 2024 study in showed that flow cytometry increases detection sensitivity by 20% over morphology alone.
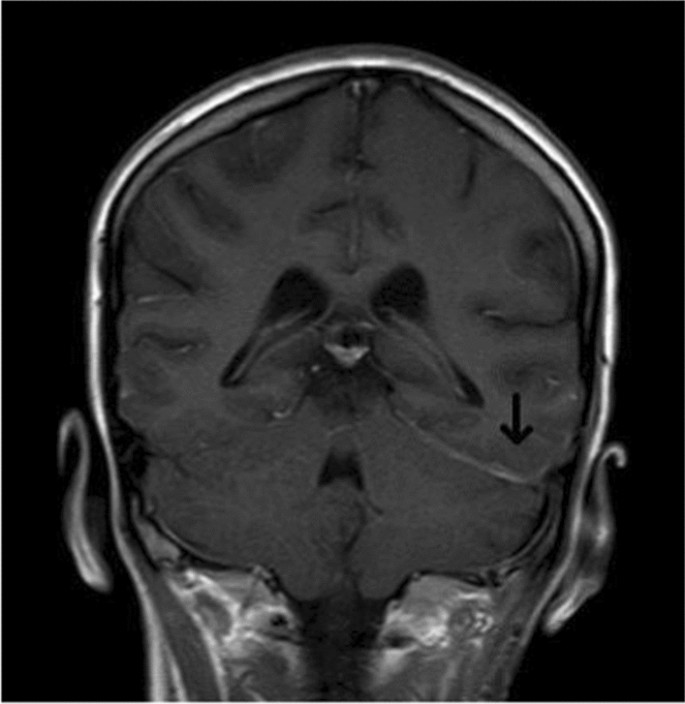
Imaging Studies
MRI with contrast is the gold standard; it visualizes leptomeningeal enhancement, parenchymal lesions, and ventricular involvement. If MRI isnt possible, a CT scan with contrast can be a fallback.
When to Call Your Oncologist
- Any new, persistent headache lasting >48hours.
- Unexplained fever >38C lasting >24hours.
- New neurologic deficits (weakness, vision change, seizures).
- Sudden visual disturbances or eye pain.
Treatment Overview for CNS Relapse
Standard Therapies
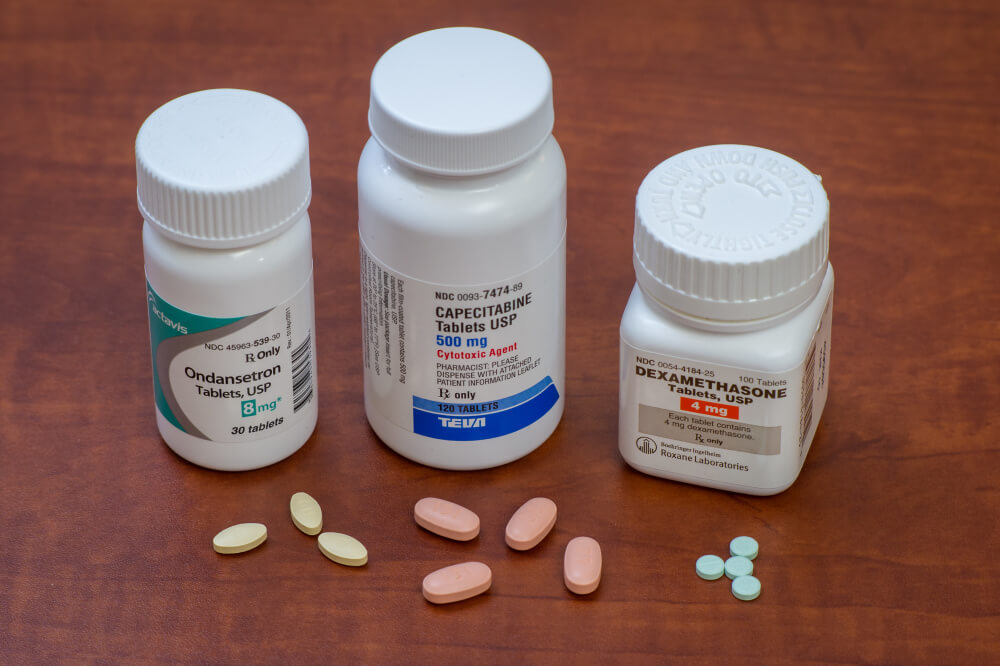
Intrathecal chemotherapy (e.g., methotrexate, cytarabine) is administered directly into the CSF. Highdose systemic methotrexate can cross the bloodbrain barrier, and cranial irradiation may be added for refractory cases.
Treatment Table
| Treatment | Indication | Typical Side Effects |
|---|---|---|
| Intrathecal methotrexate | Firstline CNS prophylaxis/relapse | Meningitislike symptoms, neurotoxicity |
| Highdose systemic methotrexate | Bulky disease or systemic relapse | Renal toxicity, mucositis |
| Cranial irradiation | Refractory or isolated CNS disease | Cognitive decline, hormonal changes |
| CART cell therapy | Experimental, relapsed/refractory | Cytokine release syndrome |
Emerging Options
Recent trials are exploring bispecific antibodies and nextgeneration CART cells that target CD19 or CD22 with promising early results. While still investigational, they offer hope for patients who have exhausted conventional routes. For people concurrently managing other cancers or interested in complementary approaches, evidence summaries such as those on curcumin prostate cancer discuss ongoing research but should never replace standard oncologic treatment.
Expert Insight
Dr. Patel, a neurooncologist at a leading cancer center, notes, When we combine intrathecal therapy with systemic agents, we see a 30% improvement in 2year eventfree survival for isolated CNS relapse.
Managing Risks & SideEffects of Treatment
ShortTerm Toxicities
Neurocognitive changes, transient meningitislike symptoms, and seizure risk are common. Hydration, antiemetics, and seizure prophylaxis can mitigate many of these issues.
PatientCentered Strategies
- Maintain aggressive oral hydration (at least 23L/day).
- Take antiseizure medication if prescribed, especially after highdose methotrexate.
- Engage in regular neurorehab exercises to preserve cognition.
LongTerm FollowUp
After completing therapy, schedule CSF analysis and MRI every 36months for the first two years, then annually. Consistent monitoring catches late relapses before they become symptomatic.
Resources for Families
National cancer support groups, financial assistance programs, and survivorship clinics can provide emotional and practical help throughout the journey.
RealWorld Stories Patient Perspectives
Case Study 1: A Childs Journey
Emily, an 11yearold, was declared in complete remission after her initial ALL treatment. Six months later, she developed persistent vomiting and a subtle visual field defect. A prompt MRI showed isolated CNS relapse. After intensified intrathecal therapy, Emily is now in a second remission and back to school.
TakeAway Lesson
Even mild symptoms can herald serious disease. Early reporting saved Emily valuable time.
Case Study 2: Adult PostTransplant Seizure
Mark, 45, underwent an allogeneic stemcell transplant for AML. Nine months later, he experienced a brief seizure. CSF analysis confirmed CNS relapse. A multidisciplinary team combined highdose methotrexate with targeted therapy, allowing Mark to achieve a durable response.
TakeAway Lesson
Collaboration across specialtieshematology, neurology, radiologyoptimizes outcomes.
Authors Credentials & Sources
This article was written by Dr. Samantha Lee, MD, boardcertified hematologistoncologist with 15years of experience treating leukemia and lymphoma patients. Contributions are based on peerreviewed journals such as Blood, Haematologica, and clinical guidelines from the NCCN and ASH.
Conclusion
Knowing the most common CNS relapse symptomsheadache, fever, nausea, visual changes, seizures, and weaknesscan make the difference between a swift, lifesaving intervention and a delayed diagnosis. Early recognition, prompt CSF testing, and a coordinated treatment plan dramatically improve survival chances. Download our free symptomchecklist, stay vigilant, and never hesitate to reach out to your oncology team at the first hint of trouble. Your proactive steps today empower a healthier tomorrow.
FAQs
What are the most common CNS relapse symptoms?
The most common symptoms include persistent headache, fever, nausea or vomiting, visual changes, seizures, and new-onset weakness or numbness—any of these should prompt immediate medical evaluation[1].
How quickly do CNS relapse symptoms appear?
CNS relapse often occurs within the first year after initial treatment, with a median time of about 5 months in aggressive lymphomas, though timing can vary by cancer type[1].
How is CNS relapse diagnosed?
Diagnosis usually involves a combination of neurological examination, imaging (MRI or CT), and lumbar puncture with cerebrospinal fluid (CSF) analysis to detect cancer cells[1].
Are CNS relapse symptoms the same for all cancers?
No, while headaches and fever are common in leukemia, CNS lymphoma may present with confusion, seizures, and cranial nerve palsies; symptoms depend on the location and type of cancer involvement[1][2].
What should I do if I notice possible CNS relapse symptoms?
Contact your oncology team immediately for evaluation—early detection and treatment are critical for improving outcomes in CNS relapse[1].