Quick Overview
What is secondary AML from MDS?
Secondary AML from MDSor sAMLis a form of acutemyeloid leukemia that arises after a prior diagnosis of MDS. Unlike denovo AML, which appears without a preexisting blood disorder, sAML carries the genetic baggage of the earlier MDS cells. This makes it harder to treat and often shortens life expectancy.
Why should you care right now?
Even lowrisk MDS carries a roughly 5% chance of transforming into sAML each year, and the risk climbs sharply in higherrisk categories. Knowing the odds lets you stay alert, discuss preventative strategies with your hematologist, and act quickly if warning signs appear.
Key Statistic Snapshot
| Risk Category | Annual Transformation Rate | Median Time to sAML (months) |
|---|---|---|
| Lowrisk MDS | 5% | 1824 |
| Intermediaterisk MDS | 12% | 1218 |
| Highrisk MDS | 25% | 812 |
These numbers come from a 2024 metaanalysis published in , which pooled data from more than 4,000 patients.
From MDS to sAML
What triggers the transformation?
Think of MDS cells as rebellious teenagersthey already have abnormal chromosomes, but they havent yet graduated to fullblown leukemia. A few more genetic hitslike mutations inTP53,RUNX1, orASXL1push them over the edge. Some of these hits are spontaneous, while others are caused by prior chemotherapy or radiation, which is why we also hear the term therapyrelated AML.
How long does it usually take?
Most people who develop sAML do so within 1224months after their MDS diagnosis, though the timeline can stretch out to five years in very lowrisk cases. The speed of progression depends on the underlying genetic changes and how aggressively the MDS was being treated.
Latency Comparison
| Risk Level | Typical Latency (months) | Common Mutations |
|---|---|---|
| Lowrisk | 2460 | SF3B1, DNMT3A |
| Intermediate | 1224 | ASXL1, RUNX1 |
| Highrisk | 612 | TP53, FLT3ITD |
Whats the most common secondary cancer after AML?
When AML itself follows another primary cancer, the most frequent sibling malignancy is chronic lymphocytic leukemia (CLL). But in the context of MDS, the most common secondary cancer is actually the sAML were discussinga logical, if grim, progression.
Spotting Symptoms
What are the hallmark signs of secondary AML?
Because sAML is essentially a faster, more aggressive version of the original MDS, symptoms can appear suddenly and be more severe. Keep an eye out for:
- Unexplained fatigue that wont improve with rest
- Easy bruising or bleeding from gums, nose, or tiny cuts
- Frequent fevers or infections that dont respond to antibiotics
- Shortness of breath, even during light activity
- Sudden weight loss or loss of appetite
These are the classic secondary acute myeloid leukemia symptoms they overlap with secondary leukemia symptoms of other subtypes, but the rapid drop in blood counts is a hallmark for AML.
How do they differ from regular MDS symptoms?
MDS usually causes mild anemia, occasional infections, and a slowgrowing tendency to bleed. When those problems worsen dramatically over weeks rather than months, youve probably entered the AML zone. In other words, the difference is the speed and severity of the drop in blood cell production.
Quick Symptom Checklist
Print this on your fridge and tick any new changes:
- [ ] New or worsening fatigue
- [ ] Unexplained bruises or petechiae
- [ ] Fevers >38C lasting >48hrs
- [ ] Shortness of breath at rest
- [ ] Rapid weight loss (5% in a month)
Survival Numbers
What is the current secondary AML survival rate?
Across major cancer registries, the fiveyear overall survival for sAML hovers around 30%. Median overall survival (OS) is often quoted as 612months, especially for patients over 60 or those with highrisk cytogenetics. This is notably lower than the ~45% fiveyear survival seen in denovo AML, underscoring the extra challenge posed by the prior MDS.
How does secondary leukemia survival compare to other secondary leukemias?
Therapyrelated AML (tAML) a subset of secondary leukemia that follows exposure to chemotherapy for another cancer shows a comparable survival range (2035%). The key driver of outcomes is the genetic profile rather than the exact origin story.
What influences life expectancy from MDS to AML?
Age, performance status, and specific mutations (especially TP53) are the biggest prognostic factors. For example, a 55yearold with lowrisk MDS who develops sAML but retains a normalkaryotype may have a mDS to AML life expectancy of up to 23 years with modern treatment, while a 75yearold with TP53mutated disease may only have a few months.
Survival by Age Group (illustrative)
| Age | Median OS (months) | Typical Treatment Approach |
|---|---|---|
| 60 | 1218 | Intensive chemo+possible transplant |
| 6170 | 812 | Venetoclaxazacitidine or clinical trial |
| >70 | 48 | Lowintensity hypomethylating agents |
Treatment Options
What are the standard secondary AML treatments?
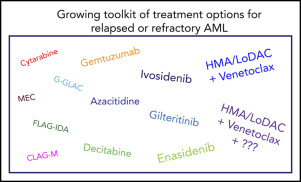
The traditional backbone has been intensive 7+3 chemotherapy (cytarabine + an anthracycline). However, because sAML patients often have poorer organ function, many clinicians now start with hypomethylating agents (HMAs) like azacitidine or decitabine, sometimes combined with the BCL2 inhibitor venetoclax. This combo has shown remission rates up to 70% in older patients.
Are there targeted therapies for secondary AML?
Yes! If molecular testing reveals FLT3ITD, IDH1/2 mutations, or other actionable changes, you can add a targeted inhibitor (midostaurin for FLT3, ivosidenib for IDH1, enasidenib for IDH2). These drugs are often used alongside HMAs, and theyve improved both response depth and durability in recent trials.
When is a stemcell transplant an option?
Allogeneic hematopoietic stemcell transplant (alloHSCT) remains the only potentially curative therapy for sAML. Eligibility hinges on age (usually 70years), comorbidities, donor availability, and the diseases genetic risk. If youre a good candidate, transplant can push fiveyear survival up to 4050%.
DecisionTree for Transplant Eligibility
- Age<70&good organ functionProceed to donor search.
- Highrisk cytogenetics (TP53)Consider clinical trial before transplant.
- No suitable donorExplore haploidentical or cordblood options.
How does prior chemotherapy affect treatment?
Patients whose sAML follows prior chemotherapy for another cancer (often called secondary leukemia after chemotherapy) may have additional organ damage that limits intensive regimens. In those cases, lowintensity HMAbased therapy is typically preferred, and clinicaltrial enrollment becomes especially valuable.
Quality of Life
What sideeffects should I expect?
Intensive chemo can cause severe neutropenia (risk of infection), mucositis (mouth sores), and alopecia (hair loss). HMAs tend to be gentler, but still cause fatigue, low blood counts, and occasional nausea. Venetoclax adds a risk of tumor lysis syndrome, which doctors mitigate with careful dosing.
How can I stay emotionally strong?
Dealing with sAML is emotionally exhausting, and its perfectly normal to feel scared or angry. Reach out to patientadvocacy groups like the Leukemia & Lymphoma Society or the MDS Foundationthey offer counseling hotlines, peertopeer forums, and financialaid guidance. Sharing your story, even just with a close friend, can lighten the mental load.
What does a typical monitoring schedule look like?
After diagnosis, youll usually have blood work weekly for the first month, then biweekly to monthly once counts stabilize. Bonemarrow biopsies are performed at baseline, after the first treatment cycle, and then every 36months to assess remission status.
Sample Monitoring Calendar (downloadable PDF)
Many cancer centers provide a printable calendar; ask your nurse for a copy so you can keep track of labs, appointments, and medication refills.
Bottom Line
Secondary AML from MDS is a serious turn in the cancer journey, slashing survival odds and demanding vigilant monitoring. Yet the story isnt all doomearly detection of hallmark symptoms, a personalized treatment plan that may blend hypomethylating agents, targeted drugs, and possibly a stemcell transplant, can meaningfully extend both lifespan and quality of life. If you notice any new bruising, fatigue, or fevers, reach out to your hematologist right away. Talk about clinicaltrial options; they often provide access to cuttingedge therapies that arent yet standard.
For patients juggling other cancer concerns, learning about related survivorship topics can be helpfulfor example, men considering prostate surgery often ask about prostate removal life expectancy to weigh longterm implications alongside blood cancer treatments.
We hope this guide gives you confidence to ask the right questions, stay proactive, and feel less alone on this path. If you have personal experiences or questions, feel free to share them with your care teamtheyre there to help you navigate every twist and turn.
FAQs
What causes secondary AML from MDS?
Secondary AML from MDS occurs when genetic mutations in MDS cells, such as TP53, RUNX1, or ASXL1, lead to progression from myelodysplastic syndrome to acute myeloid leukemia.
How quickly does MDS transform into secondary AML?
Transformation usually happens within 12 to 24 months after MDS diagnosis, with faster progression in higher-risk cases and slower in low-risk MDS patients.
What are the common symptoms signaling secondary AML?
Symptoms include worsening fatigue, easy bruising or bleeding, persistent fevers, infections, shortness of breath, and rapid weight loss, reflecting a sharp decline in blood counts.
What treatments are available for secondary AML from MDS?
Treatment options include intensive chemotherapy (7+3 regimen), hypomethylating agents combined with venetoclax, targeted therapies for specific mutations, and allogeneic stem cell transplant.
What is the survival outlook for patients with secondary AML from MDS?
The five-year survival rate for secondary AML from MDS is around 30%, which is lower than de novo AML, with outcomes depending significantly on age, genetics, and treatment received.