Why Guidelines Matter
First off, why should anyone care about a set of guidelines? Simply put, theyre the compass you need when the medical landscape feels like a stormy sea. The latest blend years of research, clinical experience, and patient stories into a single, trustworthy playbook. When you follow them, you get:
- Clear criteria for spotting the disease early because catching it sooner can save lives.
- Balanced advice on the benefits of treatment versus the risks of overtreatment.
- A realistic view of when a liver transplant is on the table and when it isnt.
Think of it as a friend whos been through the same journey and is handing you their notebook full of hardearned lessons.
Diagnostic Criteria Updated
What Exactly Counts as Portopulmonary Hypertension?
The heart of the matter (pun intended) is how doctors confirm the diagnosis. The 2024 guidelines tighten the definition to three core numbers measured during a rightheart catheterisation:
- Mean pulmonary arterial pressure (mPAP)25mmHg
- Pulmonary vascular resistance (PVR)>3 Wood units
- Pulmonary capillary wedge pressure (PCWP)15mmHg
If you see all three, youve got portopulmonary hypertension (POPH). But theres a twist: an mPAP45mmHg is now considered a hard stop for liver transplantation a crucial red flag for patients hoping for a new liver.
How Do Doctors Spot It First?
Most clinicians start with a simple transthoracic echocardiogram. If the tricuspid regurgitation (TR) jet velocity exceeds 2.8m/s, thats a cue to move on to the goldstandard test the rightheart catheter.
Quick Comparison Old vs. New Thresholds
| Parameter | Pre2022 Guideline | 2024 ILTS Guideline |
|---|---|---|
| mPAP | 25mmHg (diagnosis) | 25mmHg (diagnosis) 45mmHg (contraLT) |
| PVR | >3WU | >3WU (same) |
| PCWP | 15mmHg | 15mmHg (same) |
What Role Does Imaging Play?
While catheterisation tells you the numbers, radiology paints the picture. A chest CT or MRI can reveal:
- Enlarged pulmonary arteries
- Rightventricular hypertrophy
- Signs of coexisting hepatopulmonary syndrome (HPS)
Seeing both the pressure and the structure helps doctors decide how aggressive treatment should be. For patients also dealing with liver-related issues like fatty liver, it's helpful to understand family risks; resources on family fatty liver can provide context about hereditary factors that sometimes accompany advanced liver disease.
Understanding Pathophysiology
Why Do Liver Problems Affect the Lungs?
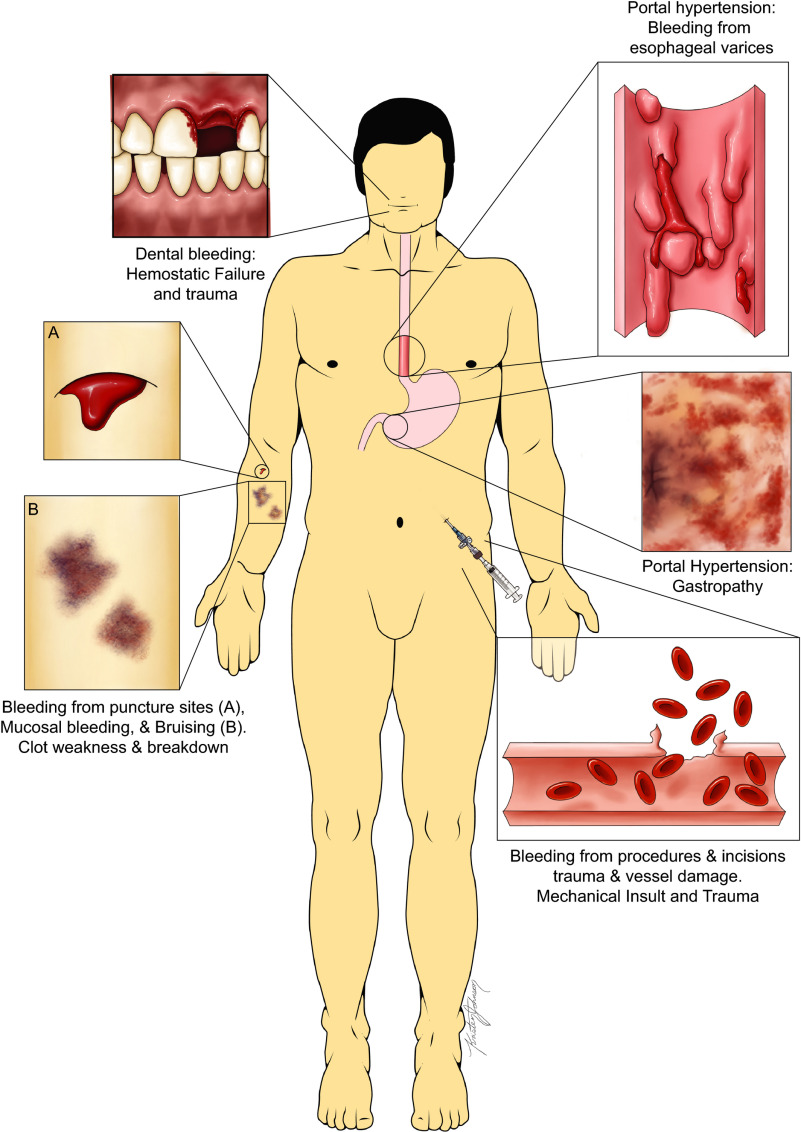
It sounds like a wild plot twist, but the connection makes sense once you consider the circulatory overload in advanced liver disease. Portal hypertension creates a hyperdynamic state the bodys blood flow ramps up, and that extra push hits the delicate vessels in the lungs. Over time, the pulmonary arteries stiffen, endothelin1 spikes, and nitric oxide dwindles, leading to the high pressures we call portopulmonary hypertension.
Is This the Same as Hepatopulmonary Syndrome?
Not exactly. POPH is a true precapillary pulmonaryarterial hypertension, whereas HPS is characterized by intrapulmonary vascular dilatations that cause low oxygen levels (hypoxemia). Some patients can have both conditions, making the treatment plan trickier. The guidelines stress that distinguishing them is key because a therapy that lowers pressure in POPH might worsen oxygenation in HPS.
Infographic Idea (for the full article)
Imagine a simple diagram that shows Portal Hypertension Blood Flow Pulmonary Artery Stress RightVentricular Overload. It would make the complex physiology feel as clear as a sunny day.
Treatment Options Explained
FirstLine Medications
When the numbers cross the threshold, medication is the first line of defence. The most commonly recommended agents are:
- Endothelinreceptor antagonists (e.g., bosentan, macitentan) great for lowering pressure but require regular liverfunction testing.
- PDE5 inhibitors (e.g., sildenafil, tadalafil) oral, easy to take, and work well in many patients.
Pros & Cons at a Glance
| Drug | Benefit | SideEffects | Monitoring |
|---|---|---|---|
| Bosentan | Improves mPAP, PVR | Hepatotoxicity, edema | Liver enzymes q3mo |
| Sildenafil | Quick oral relief | Hypotension, visual changes | Blood pressure, vision check |
When One Drug Isnt Enough
About a third of patients dont hit the target mPAP<35mmHg with monotherapy. Thats where combination therapy shines pairing an endothelin antagonist with a PDE5 inhibitor can push pressures down further, based on a 2024 multicenter trial that showed a 20% improvement in transplant eligibility.
Stories From the Front Line
Take Mike, a 52yearold with alcoholrelated cirrhosis. He started on bosentan, but his pressure stayed stubbornly high at 38mmHg. Adding sildenafil finally nudged his mPAP to 31mmHg, opening the door for a liver transplant evaluation. Real stories like Mikes remind us that one size fits all rarely applies in medicine.
Liver Transplant The Ultimate Decision
Transplantation can be lifesaving, but the guidelines set clear thresholds:
- If mPAP drops below 35mmHg after therapy, youre generally eligible.
- mPAP45mmHg is a contraindication unless you can dramatically lower it.
In practice, this means a cycle of treatment reevaluation (usually 36months later) transplant listing decision. The process is rigorous, but it also offers a realistic hopeful path.
Practical Management Steps
StepbyStep Flowchart (in words)
- Screen Annual echocardiogram for anyone with MELD12 or signs of portal hypertension.
- Confirm Rightheart catheter if echo suggests POPH.
- Clear criteria for spotting the disease early because catching it sooner can save lives.
- Balanced advice on the benefits of treatment versus the risks of overtreatment.
- A realistic view of when a liver transplant is on the table and when it isnt.
- Mean pulmonary arterial pressure (mPAP)25mmHg
- Pulmonary vascular resistance (PVR)>3 Wood units
- Pulmonary capillary wedge pressure (PCWP)15mmHg
- Enlarged pulmonary arteries
- Right-ventricular hypertrophy
- Signs of coexisting hepatopulmonary syndrome (HPS)
- Endothelin-receptor antagonists (e.g., bosentan, macitentan) great for lowering pressure but require regular liver-function testing.
- PDE5 inhibitors (e.g., sildenafil, tadalafil) oral, easy to take, and work well in many patients.
- If mPAP drops below 35mmHg after therapy, youre generally eligible.
- mPAP45mmHg is a contraindication unless you can dramatically lower it.
- Screen Annual echocardiogram for anyone with MELD12 or signs of portal hypertension.
- Confirm Right-heart catheter if echo suggests POPH.
- Stratify Group patients by mPAP: <25mmHg (no POPH), 2534mmHg, 3544mmHg, 45mmHg.
- Treat Start with a first-line vasodilator; consider combination for higher pressures.
- Reevaluate Repeat catheterisation in 36 months after therapy changes.
- Transplant Decision If mPAP<35mmHg, proceed with transplant workup; if 45mmHg, focus on aggressive medical management.
- Bloodwork (LFTs, BNP) every 13 months while on endothelin antagonists.
- Echocardiogram every 612 months, or sooner if symptoms change.
- Right-heart catheterisation at least once after therapy adjustment.
- Sudden worsening of shortness of breath or fatigue.
- Syncope (fainting) episodes.
- Rapid increase in NYHA functional class.
- Rising BNP levels or unexplained ascites.
- The full (the gold standard).
- AASLD Quick Tips for portal-hypertension screening (available on their website).
- American College of Cardiology overview of POPH (great for quick refresher).
Imagine youve just received a routine liver checkup and the doctor mentions portopulmonary hypertension. You probably think, Is that another scary term? The good news is that the portopulmonary hypertension guidelines are here to clear the fog, give you a clear road map, and even bring a bit of hope. In the next few minutes well walk through what the guidelines say, why they matter, and how you (or someone you love) can navigate diagnosis, treatment, and even liver-transplant options with confidence.
Why Guidelines Matter
First off, why should anyone care about a set of guidelines? Simply put, theyre the compass you need when the medical landscape feels like a stormy sea. The latest blend years of research, clinical experience, and patient stories into a single, trustworthy playbook. When you follow them, you get:
Think of it as a friend whos been through the same journey and is handing you their notebook full of hard-earned lessons.
Diagnostic Criteria Updated
What Exactly Counts as Portopulmonary Hypertension?
The heart of the matter (pun intended) is how doctors confirm the diagnosis. The 2024 guidelines tighten the definition to three core numbers measured during a right-heart catheterisation:
If you see all three, youve got portopulmonary hypertension (POPH). But theres a twist: an mPAP45mmHg is now considered a hard stop for liver transplantation a crucial red flag for patients hoping for a new liver.
How Do Doctors Spot It First?
Most clinicians start with a simple transthoracic echocardiogram. If the tricuspid regurgitation (TR) jet velocity exceeds 2.8m/s, thats a cue to move on to the gold-standard test the right-heart catheter.
Quick Comparison Old vs. New Thresholds
| Parameter | Pre-2022 Guideline | 2024 ILTS Guideline |
|---|---|---|
| mPAP | 25mmHg (diagnosis) | 25mmHg (diagnosis) 45mmHg (contraLT) |
| PVR | >3WU | >3WU (same) |
| PCWP | 15mmHg | 15mmHg (same) |
What Role Does Imaging Play?
While catheterisation tells you the numbers, radiology paints the picture. A chest CT or MRI can reveal:
Seeing both the pressure and the structure helps doctors decide how aggressive treatment should be. If you or your care team are also managing liver-related issues in the family, resources about family fatty liver can be helpful for broader family screening and counseling.
Understanding Pathophysiology
Why Do Liver Problems Affect the Lungs?
It sounds like a wild plot twist, but the connection makes sense once you consider the circulatory overload in advanced liver disease. Portal hypertension creates a hyperdynamic state the bodys blood flow ramps up, and that extra push hits the delicate vessels in the lungs. Over time, the pulmonary arteries stiffen, endothelin-1 spikes, and nitric oxide dwindles, leading to the high pressures we call portopulmonary hypertension.
Is This the Same as Hepatopulmonary Syndrome?
Not exactly. POPH is a true precapillary pulmonary-arterial hypertension, whereas HPS is characterized by intrapulmonary vascular dilatations that cause low oxygen levels (hypoxemia). Some patients can have both conditions, making the treatment plan trickier. The guidelines stress that distinguishing them is key because a therapy that lowers pressure in POPH might worsen oxygenation in HPS.
Infographic Idea (for the full article)
Imagine a simple diagram that shows Portal Hypertension Blood Flow Pulmonary Artery Stress Right-Ventricular Overload. It would make the complex physiology feel as clear as a sunny day.
Treatment Options Explained
First-Line Medications
When the numbers cross the threshold, medication is the first line of defence. The most commonly recommended agents are:
Pros & Cons at a Glance
| Drug | Benefit | Side-Effects | Monitoring |
|---|---|---|---|
| Bosentan | Improves mPAP, PVR | Hepatotoxicity, edema | Liver enzymes q3mo |
| Sildenafil | Quick oral relief | Hypotension, visual changes | Blood pressure, vision check |
When One Drug Isnt Enough
About a third of patients dont hit the target mPAP<35mmHg with monotherapy. Thats where combination therapy shines pairing an endothelin antagonist with a PDE5 inhibitor can push pressures down further, based on a 2024 multicenter trial that showed a 20% improvement in transplant eligibility.
Stories From the Front Line
Take Mike, a 52-year-old with alcohol-related cirrhosis. He started on bosentan, but his pressure stayed stubbornly high at 38mmHg. Adding sildenafil finally nudged his mPAP to 31mmHg, opening the door for a liver transplant evaluation. Real stories like Mikes remind us that one size fits all rarely applies in medicine.
Liver Transplant The Ultimate Decision
Transplantation can be lifesaving, but the guidelines set clear thresholds:
In practice, this means a cycle of treatment reevaluation (usually 36 months later) transplant listing decision. The process is rigorous, but it also offers a realistic hopeful path.
Practical Management Steps
Step-by-Step Flowchart (in words)
Downloadable Checklist
For the full article you could offer a printable POPH-Checklist that readers can keep on their fridge a tiny reminder that staying on top of appointments really does matter.
Monitoring & Follow-Up
Lab & Imaging Schedule
Consistency is king. The guidelines recommend:
When to Sound the Alarm
Watch for any of these red-flag signs:
If any pop up, the next step is to call your specialist immediately early intervention can turn a scary situation into a manageable one.
Resources & Further Reading
To stay on top of new developments, you might want to explore:
Conclusion
Portopulmonary hypertension can feel like a hidden storm lurking behind liver disease, but the portopulmonary hypertension guidelines give us a clear map to navigate it. From precise diagnostic thresholds to a balanced look at medication, transplant eligibility, and ongoing monitoring, the guidance empowers patients and providers alike to make informed, compassionate decisions.
So, whats next for you? If you or a loved one have been told you have POPH, start a conversation with your hepatology-pulmonary team about the latest guidelines. Ask about screening frequency, treatment options, and the realistic path to transplantation. And remember youre not alone in this journey. Share your story, ask questions, and lets keep learning together.
FAQs
What are the diagnostic criteria for portopulmonary hypertension?
Portopulmonary hypertension is diagnosed using right-heart catheterization with these criteria: mean pulmonary arterial pressure (mPAP) ≥ 25 mmHg, pulmonary vascular resistance (PVR) > 3 Wood units, and pulmonary capillary wedge pressure (PCWP) ≤ 15 mmHg.
How is portopulmonary hypertension initially screened?
Screening usually starts with a transthoracic echocardiogram. A tricuspid regurgitation jet velocity above 2.8 m/s signals the need for confirmatory right-heart catheterization.
What medications are recommended as first-line treatment?
First-line treatments include endothelin-receptor antagonists like bosentan and macitentan, and PDE-5 inhibitors such as sildenafil and tadalafil, aimed at lowering pulmonary artery pressure.
When is liver transplantation considered for patients with portopulmonary hypertension?
Liver transplant is considered if mPAP drops below 35 mmHg after medical therapy; an mPAP ≥ 45 mmHg is a contraindication unless pressures can be reduced effectively.
How should patients with portopulmonary hypertension be monitored?
Regular follow-up includes blood tests (LFTs, BNP) every 1–3 months, echocardiograms every 6–12 months or as symptoms change, and repeat right-heart catheterization after therapy adjustments.