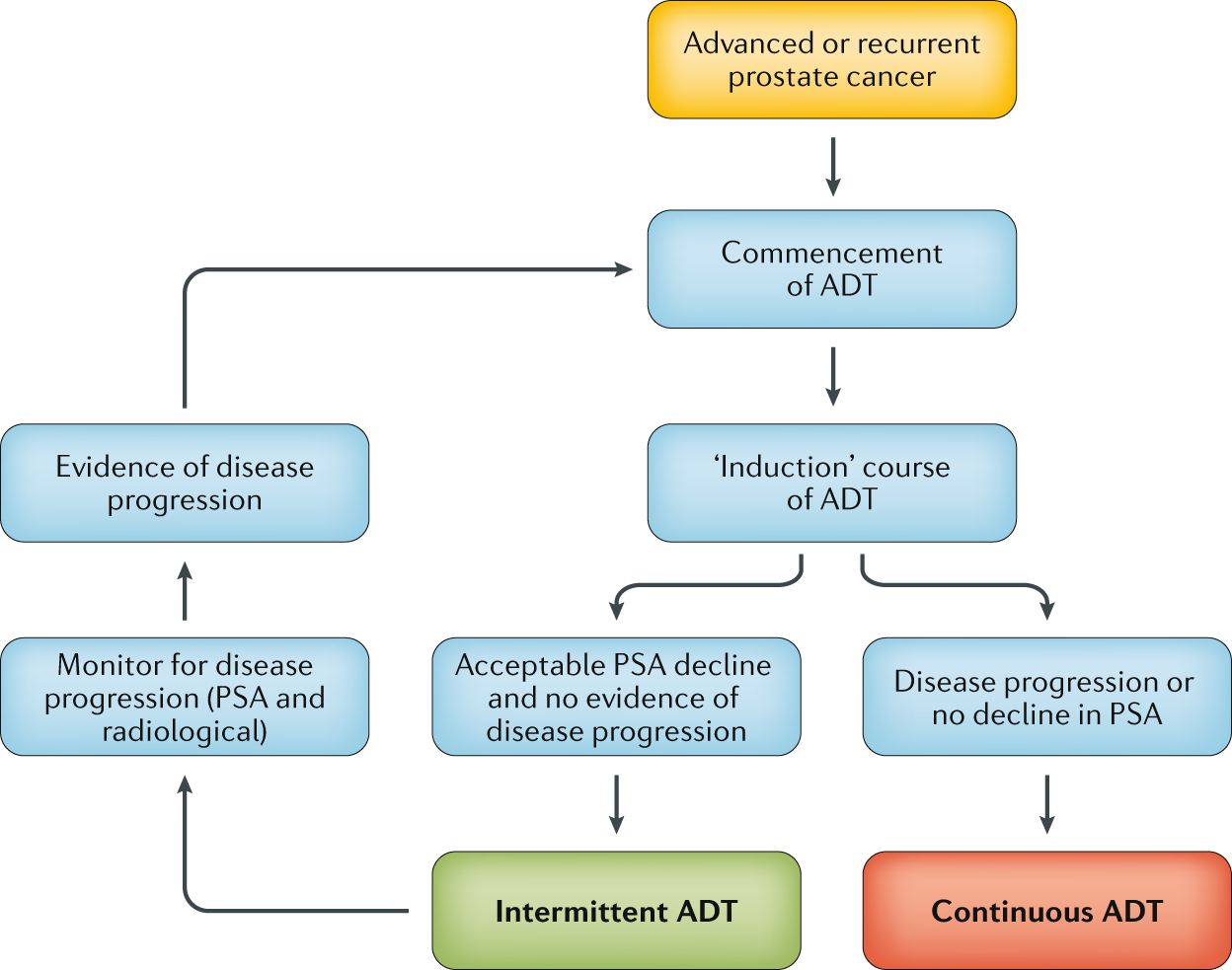
Looking for the most common androgendeprivationtherapy (ADT) options? In short, theyre injectable hormonesuppressing shots, oral antiandrogens, and newer combination regimens that pair ADT with radiation.
Each choice carries its own schedule, effectiveness, and sideeffect profile. Knowing the pros and cons helps you (or a loved one) decide what fits best with life, work, and personal comfort.
How ADT Works
What is androgendeprivation therapy?
ADT is a treatment that lowers testosteronethe hormone that fuels most prostate cancers. By cutting off that fuel, the cancer slows its growth or even shrinks.
Why does lowering testosterone matter?
Prostate cells are like cars that run on gasoline; testosterone is that gas. When the fuel is gone, the engine sputters. This is why doctors often start ADT when the cancer shows signs of spreading.
When do doctors recommend ADT?
ADT is used in several situations:
- Highrisk localized disease before radiation (neoadjuvant).
- Concurrent with radiation for intermediate or highrisk tumors.
- Metastatic disease, where its the cornerstone of treatment.
These recommendations are backed by guidelines from the and the .
Main ADT Types
Injectable LHRH agonists
These are the classic shotsgoserelin, leuprolide, and triptorelin. They trick the pituitary gland into releasing a surge of luteinisinghormone, which later shuts down, dropping testosterone dramatically.
Typical injection schedule
Most patients receive a depot injection every month, every three months, or every six months. The threemonth option is often the sweet spot for convenience and steady hormone control.
LHRH antagonists
Degarelix and the newer oral relugolix act faster because they block the receptor straight awayno initial testosterone surge.
Firstgeneration antiandrogens
Bicalutamide, flutamide, and nilutamide are taken orally and block testosterone from binding to cancer cells. Theyre usually added to an LHRH agent. For patients and caregivers wanting an overview of commonly used medicines, a plain-language guide to anti-androgens prostate cancer can be helpful.
Nextgeneration antiandrogens
Enzalutamide, apalutamide, and darolutamide are the modern oral drugs that not only block the receptor but also prevent its activation inside the cell. Theyve shown strong survival benefits in recent trials.
CYP17 inhibitors
Abiraterone acetate, taken with lowdose prednisone, blocks an enzyme needed for testosterone production not only in the testes but also in the adrenal glands.
InjectionBased ADT
How the 3month depot works
The medication is mixed with a tiny amount of oil and released slowly over roughly 90 days. This steady release is why doctors talk about prostate cancer injections every 3 months.
Common side effects right after injection
Patients often feel a brief hotflash, mild fatigue, or a little soreness at the injection site. Most of these symptoms fade within a few days.
Managing injectionsite pain
Apply a cold pack for 1015 minutes, use overthecounter NSAIDs if needed, and keep the arm moving gently. A quick stretch can also help reduce stiffness.
Frequency options: pros & cons
- Monthly: More frequent visits, but you feel the hormone drop sooner if you need to stop.
- Quarterly: Convenient, fewer trips, steady hormone levels.
- Semiannual: Best for those who travel or have busy schedules, but a missed dose can leave a longer gap.
Oral & Combo Options
When doctors add an antiandrogen
Combining an LHRH agonist with an oral antiandrogencalled combined ADThelps prevent the brief testosterone surge and offers a stronger fight against the cancer.
Specific drug profiles
Enzalutamide, for example, is taken once daily at 160mg and has shown a 30% reduction in disease progression in the PROSPER trial. Apalutamide and darolutamide have similar benefits with slightly different sideeffect patterns.
What drugs are used for androgen deprivation therapy?
| Drug | Brand | Route | Typical Dose | Key Side Effects |
|---|---|---|---|---|
| Leuprolide | Lupron | Injectable | 22.5mg q3mo | Hot flashes, bone loss |
| Degarelix | Firmagon | Injectable | 240mg loading, then 80mg qmo | Injection site reactions |
| Bicalutamide | Casodex | Oral | 50mg daily | Liver enzyme changes |
| Enzalutamide | Xtandi | Oral | 160mg daily | Fatigue, hypertension |
| Abiraterone | Zytiga | Oral | 1000mg daily + prednisone | Low potassium, liver issues |
ADT + Radiation
Evidence of improved survival
Multiple randomized trials, including a landmark study published in The Lancet, found that adding ADT to externalbeam radiation improves overall survival by up to 15% in highrisk patients.
Typical sequencing
Most clinicians start ADT 23 months before radiation (neoadjuvant), continue during the treatment (concurrent), and then maintain it for 23 years after (adjuvant). The exact length depends on risk factors and patient tolerance.
Patientcentred outcomes
While survival gains are clear, qualityoflife studies show that men on combined therapy report more fatigue and sexual changes. Thats why shared decisionmaking is essential.
Therapy Duration
How long can a man stay on hormone therapy?
Standard durations range from six months for shortterm neoadjuvant use to indefinite treatment for metastatic disease. Some highrisk localized cases receive ADT for 23years.
Risks of prolonged ADT
Longterm hormone suppression can lead to bone thinning, increased cardiovascular risk, diabetes, and mood changes. Regular bonedensity scans and hearthealth monitoring become part of routine care.
Refusing hormone therapy
Its absolutely okay to decline ADT after a thorough discussion. Reasons include concerns about side effects, desire to maintain sexual function, or personal values. In such cases, doctors may explore active surveillance or focal therapies instead.
Decisionmaking checklist
- Understand the expected survival benefit.
- Consider your lifestyle and work commitments.
- Ask about boneprotective meds (denosumab, zoledronic acid).
- Review cardiovascular health and diabetes risk.
- Talk openly about sexual health and mood.
When ADT Fails
Mechanisms of resistance
Over time, some cancers learn to grow without testosterone. They may develop AR splice variants or ramp up alternative pathways, leading to castrationresistant prostate cancer.
Nextline options
When hormone therapy stops working, options include newer antiandrogens (e.g., enzalutamide), chemotherapy (docetaxel), radiopharmaceuticals (radium223), or enrollment in a clinical trial.
Monitoring PSA trends
PSA rises are often the first clue that ADT is losing its grip. Regular PSA testing every 36 months helps catch the change early, giving you and your doctor time to adjust treatment.
SideEffect Management
Common side effects
Hot flashes, fatigue, loss of libido, and mild anemia are the usual suspects. Theyre uncomfortable but manageable in most cases.
Lifestyle tweaks
Regular aerobic exercise (30minutes, 5days a week) can improve energy and bone health. A diet rich in calcium, vitamin D, and lean protein helps protect bones. Staying cool with layered clothing or a fan eases hot flashes.
Serious risks
Longterm ADT can increase heart attack risk, cause diabetes, and lead to severe osteoporosis. Your doctor may prescribe statins, antihypertensives, or bonestrengthening agents as preventive measures.
Preventive measures
Denosumab (Prolia) or zoledronic acid are commonly used to keep bone density up. Bloodpressure checks and lipid panels become routine, especially after the first year of therapy.
Emotional & psychosocial impact
Feeling less manly can hit the confidence button hard. Support groups, counseling, or even an online forum can provide an outlet. Talking openly with a partner often eases relationship strain.
RealWorld Stories
My first 3month injection
Mark, 62, described his first leuprolide depot as a tiny poke, then a night of weird sweats that felt like a sauna. After a week, the sweats faded and he appreciated the convenience of only needing to visit the clinic quarterly.
Balancing work, family, and ADT
Saras husband, Tom, kept his job as a carpenter while on degarelix. He scheduled his injections right after a weekend trip, so the downtime never interfered with a project deadline. A simple calendar reminder saved him from missing a dose.
When I chose to stop ADT
James, 68, decided after two years that the side effects outweighed the benefits for his slowgrowing tumor. He consulted his oncologist, transitioned to active surveillance, and now enjoys hiking without the constant fatigue.
Quick Answers
What drugs are used for androgen deprivation therapy?
LHRH agonists (leuprolide, goserelin), LHRH antagonists (degarelix), firstgeneration antiandrogens (bicalutamide), nextgeneration antiandrogens (enzalutamide, apalutamide, darolutamide), and CYP17 inhibitors (abiraterone).
How long can a man stay on hormone therapy for prostate cancer?
From six months for shortterm neoadjuvant use to indefinite for metastatic disease; many highrisk localized cases receive 23years.
What are the side effects of ADT?
Hot flashes, loss of libido, fatigue, bone loss, metabolic changes, and increased cardiovascular risk.
Is ADT combined with radiation effective?
Yesclinical trials show a clear survival advantage for highrisk patients who receive both treatments.
What happens when hormone treatment stops working?
The cancer may become castrationresistant, prompting a switch to newer antiandrogens, chemotherapy, or clinical trial enrollment.
Can a patient refuse hormone therapy?
Absolutely. After a thorough discussion of benefits and risks, patients may opt for active surveillance or alternative local therapies.
Understanding the landscape of ADTfrom injectables every three months to oral combo pillsempowers you to make choices that align with your health goals and lifestyle. If anything feels overwhelming, remember youre not alone: doctors, nurses, support groups, and even friendly forums are there to guide you.
Whats your experience with ADT? Have you found a tip that made the journey easier? Share your thoughts in the commentsyour story could help someone else navigate this path with confidence.
FAQs
What are the most common injectable ADT options?
The typical injectable ADT drugs are LHRH agonists such as leuprolide, goserelin, and triptorelin, as well as LHRH antagonists like degarelix.
How often are 3‑month ADT injections administered?
These depot injections are given once every 12 weeks, providing steady testosterone suppression for about three months.
Can ADT be combined with radiation therapy?
Yes, adding ADT to external‑beam radiation improves overall survival for high‑risk prostate cancer patients.
What are the main side effects of long‑term ADT?
Prolonged hormone suppression can cause bone loss, cardiovascular risk, diabetes, hot flashes, fatigue, and reduced libido.
What oral anti‑androgens are considered next‑generation?
Enzalutamide, apalutamide, and darolutamide are modern oral agents that block the androgen receptor more completely than older drugs.