Spinal fluid leukemia means that leukemic cells have found their way into the cerebrospinal fluid (CSF) surrounding your brain and spine. Its a signal that the disease has moved beyond the bone marrow, and it can change the way doctors treat it and how the outlook looks.
Below youll get straighttothepoint answers about the symptoms you might notice, the survival odds, the treatment options, and what the journey looks like for both kids and adults. No fluffjust the information you need to feel a little less lost and a little more empowered.
How Leukemia Spreads
What is CNS leukemia?
CNS leukemia (sometimes called central nervous system leukemia) is the medical term for leukemia that has entered the CSF. Think of the CSF as the clear, protective cushion around your brain and spinal cord. When cancerous whiteblood cells slip into that space, theyre no longer confined to the marrow.
Pathways of spread
There are a couple of ways the disease can get into the spinal fluid. The most common route is through the bloodstreamleukemic blasts cross the bloodbrain barrier and settle in the CSF. Less often, the cancer grows directly into the meninges (the membranes covering the brain and spine). Either way, the meningeal environment can actually help the blasts survive longer, which is why early detection matters.
Expert insight
Dr. Laura Martinez, a pediatric hematologistoncologist at a leading cancer center, says, Routine CSF analysis at diagnosis is essential because CNS involvement can be silent. Catching it early lets us tailor therapy before symptoms flare up. Youll often see her quoted in the for leukemia.
Spotting the Symptoms
Common early signs
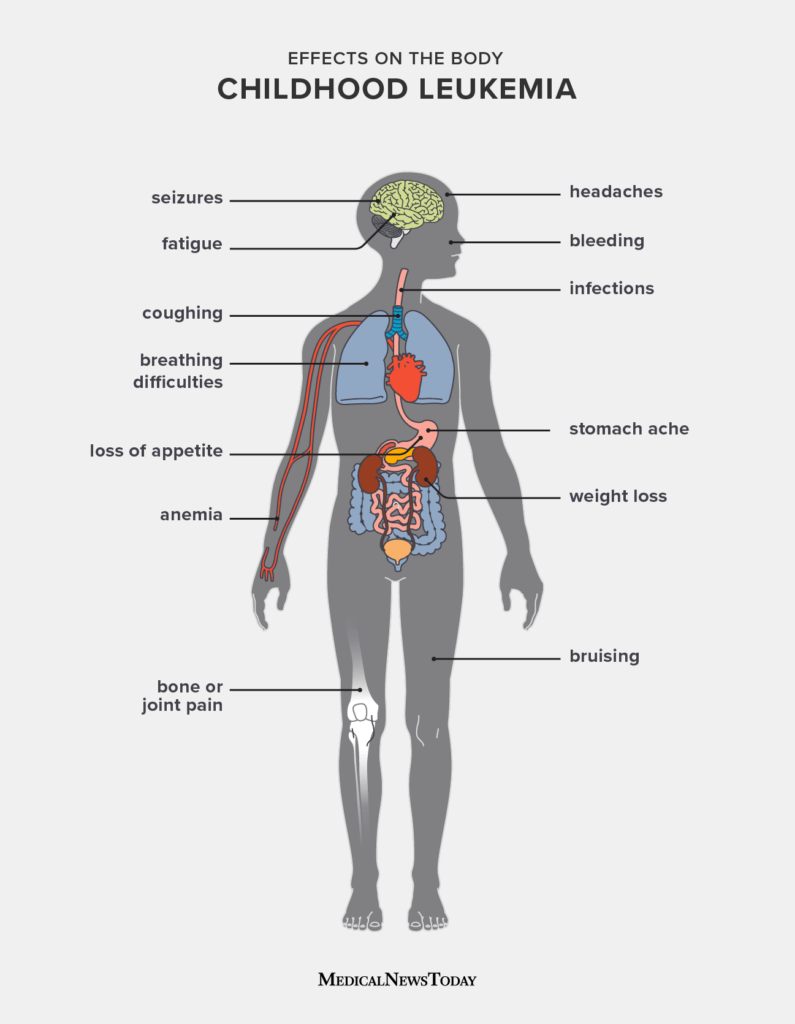
When leukemia is hanging out in the spinal fluid, the body sends warning signals. Headaches that feel worse when youre lying down, neck stiffness, blurry vision, and occasional vomiting are classic. Some people also experience seizures or sudden weakness in an arm or leg.
Kids vs. adults
Children often cant put the feeling into words. Irritability, a sudden change in feeding habits, or a regression in developmental milestones can be clues. Adults, on the other hand, might notice subtle cognitive changes, balance problems, or a fog that makes it hard to concentrate.
Why many cases are silent
Surprisingly, up to 30% of CNS involvement is discovered only because a lumbar puncture revealed blasts that werent causing any symptoms. Thats why doctors routinely check the CSF even if you feel fine.
Realworld story
Take Maya, an eightyearold diagnosed with acute lymphoblastic leukemia (ALL). She started complaining of big headaches after a weekend of playing soccer. A quick spinal tap showed leukemia in spinal fluid, and her doctors added intrathecal therapy right away. Mayas story shows how a simple symptom can change the treatment plan and improve her chances of remission.
How Its Diagnosed
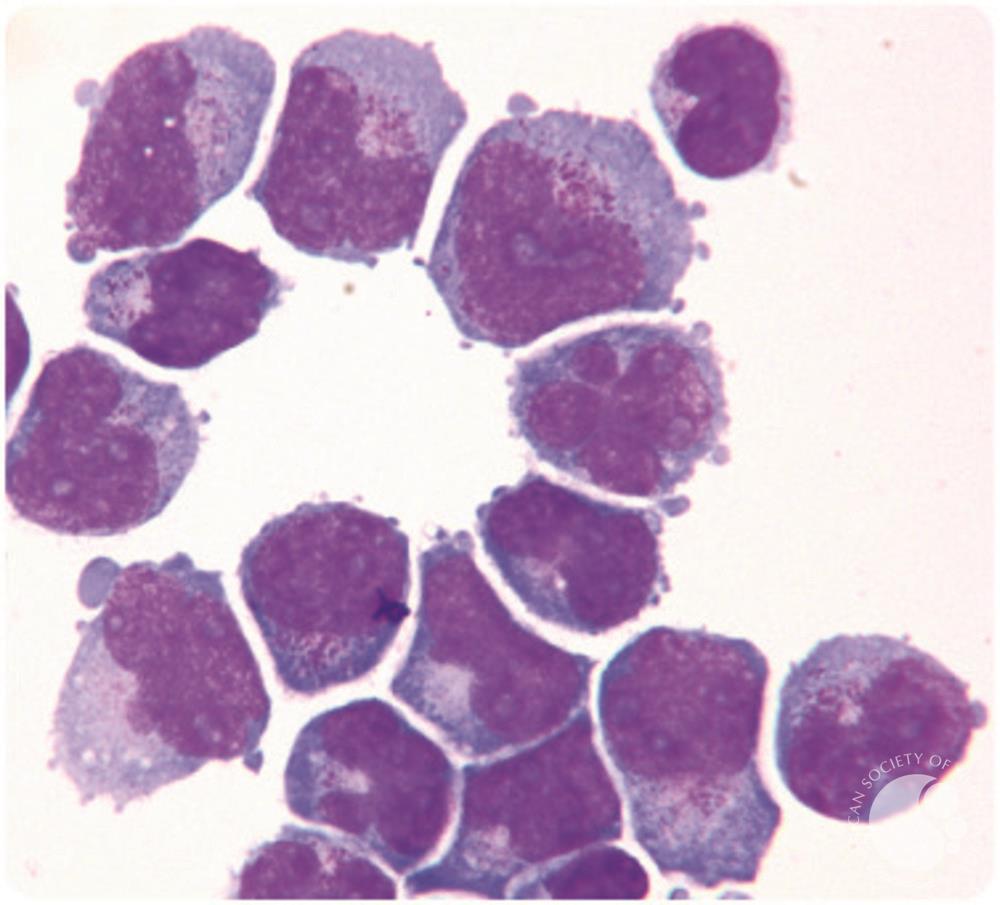
Lumbar puncture & CSF cytology
The gold standard is a lumbar puncturecommonly called a spinal tap. A thin needle draws a few milliliters of CSF, which the lab examines under a microscope (cytology) and with flow cytometry to spot leukemia cells.
Imaging aids
If neurological symptoms are prominent, an MRI of the brain and spine helps rule out mass lesions or inflammation that might be mimicking leukemia spread.
Molecular profiling
Newer labs can run nextgeneration sequencing on CSF cells, spotting mutations like FLT3ITD or IDH1 that guide targeted therapy. Its a hightech way to finetune treatment.
Reliable sources
For deeper technical details, the offers a clear overview of CSF testing in leukemia.
Survival Rates & Prognosis
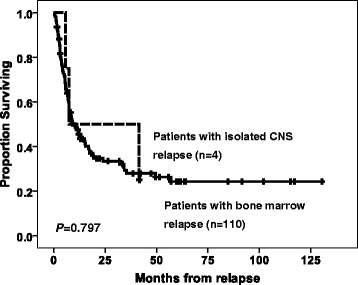
Overall survival numbers
When leukemia reaches the CSF, survival rates dip compared to marrowonly disease. For AML (acute myeloid leukemia) with CSF involvement, the fiveyear overall survival hovers around 3040%. In ALL (acute lymphoblastic leukemia), especially in kids, the numbers climb to roughly 5070% when aggressive CNSdirected therapy is used.
Key factors shaping outlook
Age, type of leukemia, the number of blasts in the CSF, genetic risk markers, and how quickly the disease responds to induction therapy all sway the prognosis. For instance, a high blast count (>5%) in the spinal fluid typically knocks a few percentage points off the survival curve.
Kids vs. adults
Children tend to fare better. Lowrisk ALL in a child can have an 80% cure rate even with CNS involvement, while adults over 60years old with AML in the spinal fluid often struggle to reach a 20% longterm survival.
Prognostic table
| Variable | Impact on Survival |
|---|---|
| CSF blast %>5% | Decrease overall survival by ~15% |
| Highrisk cytogenetics (e.g., FLT3ITD) | Further reduction in survival |
| Age>60years | Significant drop in survival odds |
| Child with lowrisk ALL | Potential cure rates ~80% |
Treatment Options
Systemic chemotherapy that reaches CSF
Highdose cytarabine and methotrexate are the workhorses that can cross the bloodbrain barrier. New agents like venetoclax are being explored for AML with CNS disease.
Intrathecal chemotherapythe backbone
Directly injecting drugs into the CSF bypasses the barrier entirely. Methotrexate, cytarabine, and sometimes a steroid are given during induction, then again in consolidation and maintenance phases. This is the cornerstone of leukemia in spinal fluid treatment.
Targeted and immunotherapy breakthroughs
For patients with specific mutations, FLT3 inhibitors (midostaurin) or IDH inhibitors can be added. In ALL, CD19directed CART cells have shown promise even when the disease is in the CNS. Ongoing trials listed on are testing these combos.
When radiation steps in
Radiation isnt the first line, but it saves lives when the leukemia is stubborn, such as after multiple intrathecal rounds fail or when theres a bulky meningeal mass.
Stemcell transplant for highrisk cases
Allogeneic stemcell transplantation offers the best chance for durable remission in adults with AML and CNS involvement, though it carries its own risks.
Patientfocused care checklist
- Baseline CSF assessment before starting therapy.
- Premedication with steroids to reduce chemical meningitis.
- Hydration and antiemetics to manage side effects.
- Regular neurological exams and repeat lumbar punctures to track response.
- Access to psychosocial supportcounseling, support groups, survivorship programs.
Managing Side Effects & Quality of Life
Common toxicities of intrathecal drugs
Patients sometimes experience chemical meningitisa painful headache and neck stiffness that mimic infection. Rarely, neurotoxicity can lead to numbness or weakness.
Supportive measures
Staying wellhydrated, taking prescribed antiseizure meds if needed, and using gentle stretching can ease discomfort. Many centers give a short course of dexamethasone before each intrathecal dose to blunt inflammation.
Longterm followup
Even after remission, survivors often need neurocognitive testing, endocrine evaluations, and regular MRI scans to catch late effects early. Survivorship clinics specialize in these checks and provide resources for returning to school or work.
Personal anecdote
When I was a medical student shadowing an adult AML patient, Mr. Patel, he told me that after his second round of intrathecal methotrexate he felt a buzzing in his fingertips. A quick adjustment of his hydration plan and a short steroid taper cleared it up. Stories like his remind us that sideeffects are manageable when youre proactive.
Resources & Further Reading
For more detailed guidelines, you can explore the for leukemia. The also offers patient-friendly brochures and a directory of support groups worldwide. If youre looking for a community of parents navigating leukemia in spinal fluid child journeys, their online forums are a treasure trove of shared experience.
Conclusion
Spinal fluid leukemia is a serious turn in the leukemia story, but its not a deadend. Early detection, aggressive CNSdirected therapy, and a personalized treatment plan can dramatically improve outcomesespecially for children. Survival rates are lower than for marrowonly disease, yet advances in targeted drugs and immunotherapy are steadily raising hope. If you or a loved one faces this diagnosis, stay informed, ask your oncologist about CSF testing, and consider joining a survivorship program for ongoing support. Were all in this togetherfeel free to share your thoughts, ask questions, or tell us about your own experience in the comments below.
FAQs
What is spinal fluid leukemia?
Spinal fluid leukemia is when leukemia cells infiltrate the cerebrospinal fluid (CSF) that surrounds the brain and spinal cord, indicating central nervous system involvement.
How is spinal fluid leukemia diagnosed?
The diagnosis is made mainly by a lumbar puncture (spinal tap) that collects CSF for cytology, flow cytometry, and molecular testing. MRI may be added if neurological signs appear.
What symptoms suggest leukemia has spread to the CSF?
Typical signs include worsening headaches, neck stiffness, visual changes, vomiting, seizures, or sudden weakness. Children may show irritability or developmental regression.
What treatments are used for spinal fluid leukemia?
Therapy combines high‑dose systemic chemotherapy that crosses the blood‑brain barrier with intrathecal chemotherapy (methotrexate, cytarabine, steroids). Targeted agents, immunotherapy, radiation, or stem‑cell transplant are added for high‑risk cases.
How does CNS involvement affect prognosis?
Overall survival drops compared with marrow‑only disease. Children with low‑risk ALL can still achieve 70‑80 % cure rates, while adults with AML and CSF involvement often have 20‑40 % five‑year survival, depending on age, blast count and genetics.