If you or someone you love is living with acute myeloid leukemia (AML), the thought of the disease returning in the brain or spinal fluid can feel like a nightmare you cant wake up from. Below youll get the straighttothepoint facts about isolated CNS relapse AMLwhat it means, how often it shows up, the warning signs, and what doctors actually do about it.
Skip the fluff. In the next few minutes youll understand the risk, learn the symptoms to watch for, and see the realworld options that can keep you or a loved one one step ahead.
What Is Isolated
What does CNS relapse mean for AML patients?
CNS stands for central nervous system, which includes the brain, spinal cord, and the fluid (cerebrospinal fluid or CSF) that surrounds them. A relapse means leukemia cells have returned after a period of remission. When those cells are found only in the CNS and not in the bone marrow or blood, we call it an isolated CNS relapse.
Why is it called isolated?
Its isolated because the disease has resurfaced solely in the central nervous system. The rest of the bodyyour bone marrow, peripheral blood, even other organsstill look clean under the microscope.
How common is an isolated CNS relapse?
Its rare, but not negligible. Large studies report incidence rates ranging from 1% to 8% of all AML cases. In patients with the inv16 cytogenetic subtype who receive standarddose cytarabine, the rate can climb to about 30%, whereas highdose regimens drop it to near zero. For those undergoing allogeneic stemcell transplant, isolated CNS relapse appears in roughly 1.8% of cases..
Who is at highest risk?
Risk factors include:
- Inversion 16 (inv16) AML
- High whitebloodcell count at diagnosis
- Previous CNS involvement (e.g., meningeal leukemia)
- Extramedullary disease (leukemia outside bone marrow)
- Specific genetic mutations such as FLT3ITD
How Common Is It
What do recent largecohort studies say?
Below is a snapshot of the numbers youll often see in the literature:
| Study | Population | Isolated CNS Relapse Rate |
|---|---|---|
| AlloHSCT Registry (2020) | 2,045 transplant recipients | 1.8% |
| Denovo AML Cohort (2019) | 886 newly diagnosed adults | 0.9% |
| Inv16 + Standard Cytarabine (2018) | 124 patients | 30% |
| Inv16 + HighDose Cytarabine (2018) | 118 patients | ~0% |
Does treatment style affect the rate?
Yes. Highdose cytarabine, especially when combined with intrathecal (directly into the CSF) therapy, dramatically lowers the chance of a CNS relapse. Thats why many oncologists tailor prophylactic regimens for patients who carry highrisk genetic features.
Spotting Symptoms
What are the most common CNS relapse symptoms?
Leukemia hiding in the brain or spinal fluid can masquerade as everyday aches, but look out for these red flags:
- Persistent or worsening headache
- Blurred vision or double vision
- Sudden seizures, especially if youve never had them before
- Facial weakness, numbness, or difficulty speaking
- Unexplained nausea, vomiting, or loss of appetite
- Back pain that feels different from typical muscle soreness
- Changes in mental statusconfusion, drowsiness, or mood swings
How do symptoms differ from AML encephalopathy?
AML encephalopathy usually stems from metabolic imbalances, infections, or medication sideeffects and often improves when those issues are corrected. In contrast, CNS relapse is driven by leukemic cells infiltrating the nervous tissue, so symptoms tend to persist or worsen despite standard supportive care.
When should a patient call the doctor?
Any new neurologic symptom that doesnt resolve within a day or two deserves a prompt call. Better to be safe and have a professional take a look.
Getting a Diagnosis
What tests confirm CNS involvement?
The gold standard is a lumbar puncture (spinal tap) to obtain CSF. The fluid is examined by:
- Cytology (looking for leukemia blasts under a microscope)
- Flow cytometry (identifies cell surface markers)
- Polymerase chain reaction (PCR) for specific genetic mutations
ImagingMRI of the brain and spinehelps locate lesions that may not shed cells into the CSF right away.
Can imaging miss it?
Yes. MRI is sensitive for structural changes but can be normal when leukemic cells are floating in the CSF. Thats why most guidelines recommend a combined approach: symptom MRI lumbar puncture.
Do guidelines suggest a diagnostic algorithm?
According to the , the flow looks like this:
- New neurologic symptom urgent MRI
- If MRI is suspicious or symptoms persist lumbar puncture
- CSF analysis (cytology+flow) confirms or rules out relapse
Treatment Options
What are the standardofcare therapies?
Most experts start with highdose systemic cytarabine (AraC) because it penetrates the bloodbrain barrier. This is usually paired with intrathecal chemotherapydirectly injecting drugs like methotrexate, AraC, and hydrocortisone into the CSF.
When is intrathecal chemotherapy used?
Its given on a schedule such as twice a week for two weeks, then weekly, depending on response. The goal is to wash out any residual blasts lurking in the CSF.
Are targeted agents useful?
Some newer drugsFLT3 inhibitors (e.g., gilteritinib) and IDH inhibitors (enasidenib, ivosidenib)show modest ability to cross the barrier. Clinical trials are ongoing, but for now theyre considered adjuncts rather than primary therapy.
What about stemcell transplantation?
If a patient achieves remission after chemotherapy, many physicians recommend an allogeneic stemcell transplant (alloHSCT). Studies suggest a 1year overall survival of roughly 3040% after transplant for isolated CNS relapse, which is better than chemotherapy alone.
How to manage sideeffects?
Both highdose cytarabine and intrathecal drugs can cause:
- Neurotoxicitynumbness, tingling, or memory changes
- Myelosuppressionlow blood counts, raising infection risk
- Renal stressespecially with methotrexate, requiring vigorous hydration and leucovorin rescue
Close monitoring, supportive transfusions, and infection prophylaxis (antibiotics, antivirals, antifungals) are essential.
Prevention Strategies
Should every AML patient get CNS prophylaxis?
No, prophylaxis isnt routine for everyone. Its reserved for those with highrisk featureslike inv16, high WBC, or a history of CNS disease.
What prophylactic regimens are evidencebased?
Typical approaches include:
- Intrathecal AraC (12mg) administered weekly for 46 weeks during induction
- Highdose systemic cytarabine (13g/m) given in multiple cycles
One prospective trial showed that combining both reduced isolated CNS relapse to virtually zero in the inv16 subgroup.
Are there downsides to prophylaxis?
Yesadditional lumbar punctures can be uncomfortable, and highdose cytarabine carries a higher risk of cerebellar toxicity, especially in older adults. Balancing benefit vs. risk is a shared decision between patient and oncologist.
How do clinicians decide?
They use a decisiontree based on age, genetic risk, initial leukocyte count, and any prior CNS involvement. If two or more highrisk markers are present, prophylaxis is usually recommended.
RealWorld Stories
Case example: Isolated CNS relapse after induction
John, a 42yearold with inv16 AML, completed standard induction and felt greatuntil he started having severe headaches and double vision a month later. An MRI was equivocal, but a lumbar puncture revealed 25% blasts in his CSF. He received intrathecal AraC plus highdose systemic cytarabine and subsequently had an alloHSCT. At twoyear followup, his disease remains in remission.
Patient testimonial: I thought I was cured
When the headaches began, I brushed them off as stress from work, says Maria, 58. But the nausea wouldnt go away. My doctor ordered a spinal tap, and thats when we discovered the relapse. The treatment was tough, but knowing exactly what was happening gave me confidence to fight.
What clinicians learned
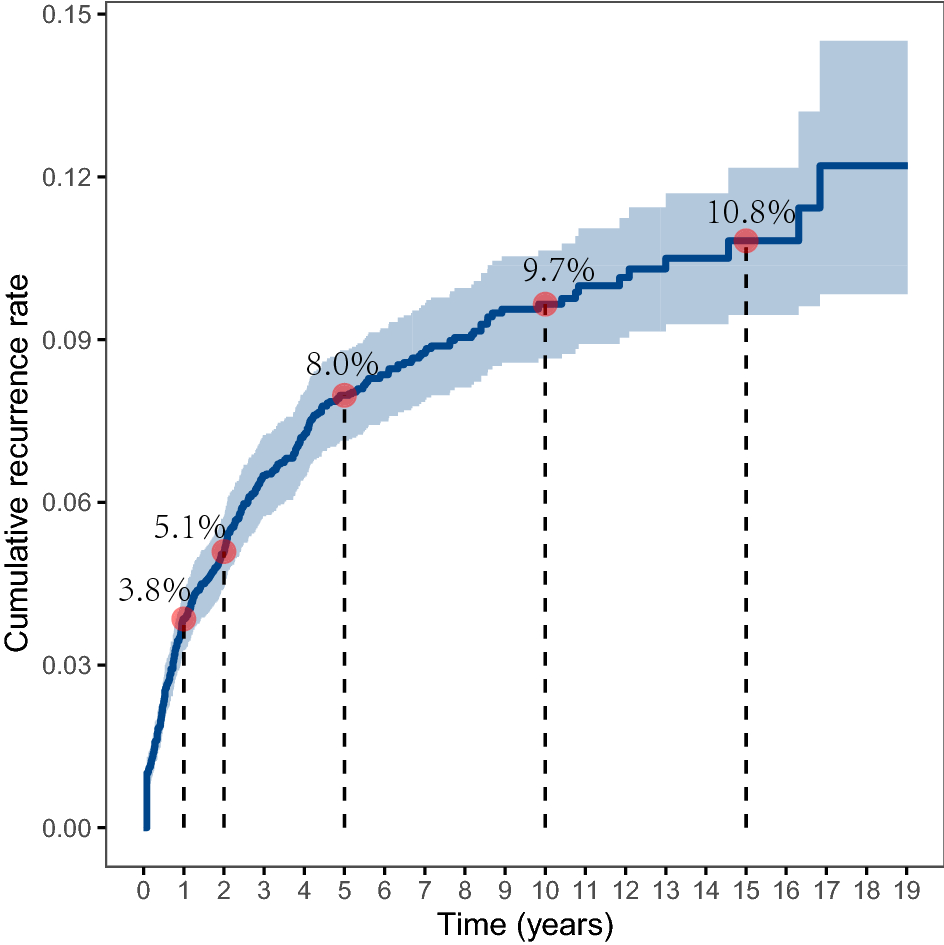
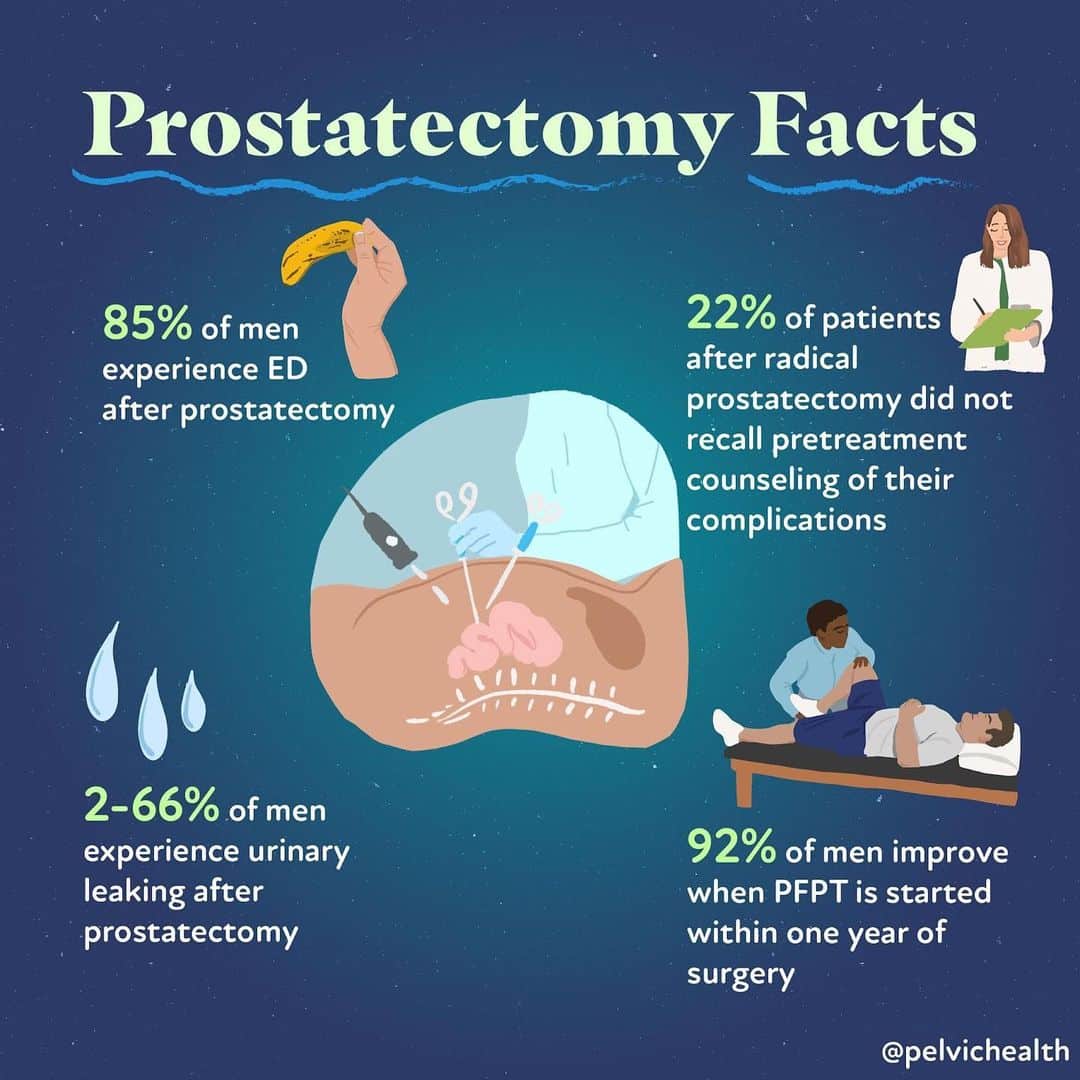
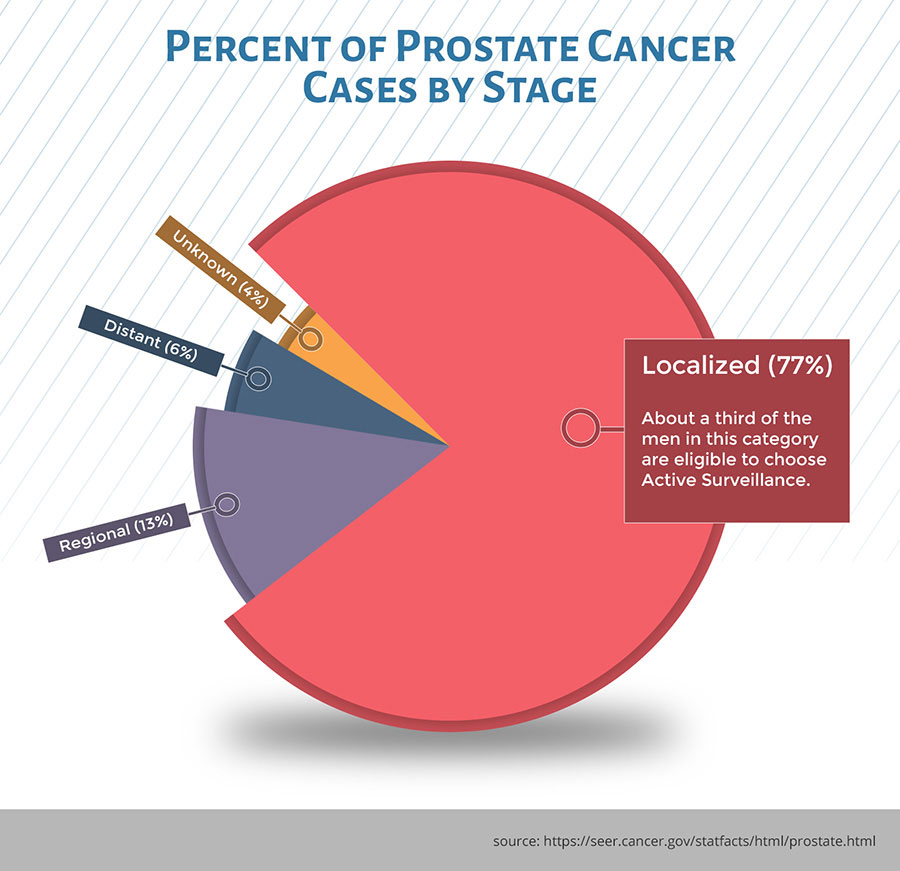
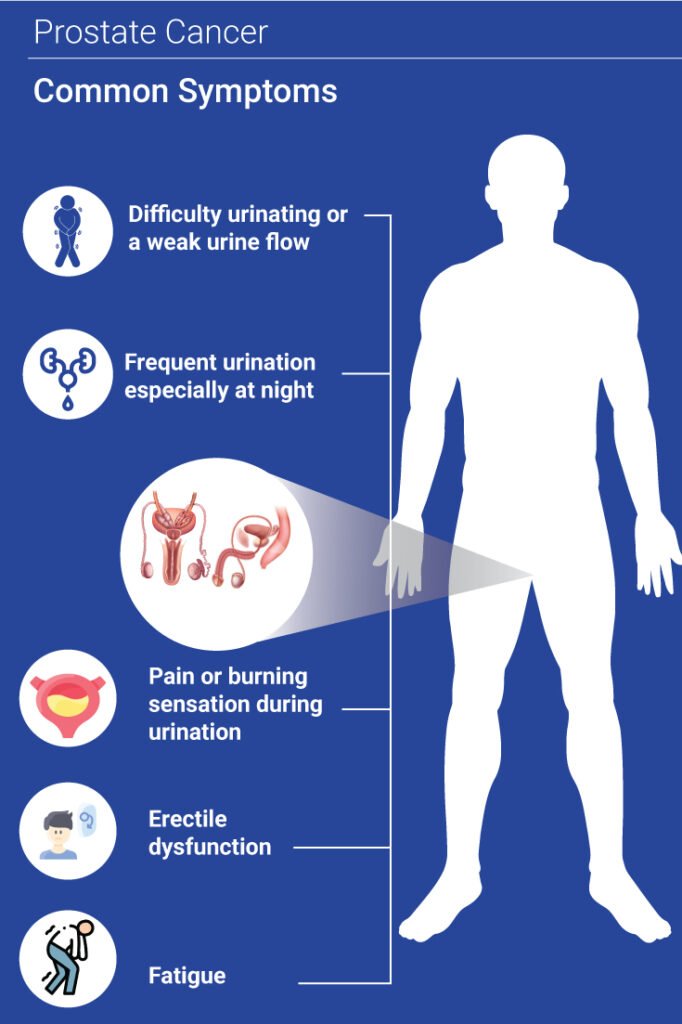
Both stories highlight the value of early CSF analysis whenever neurologic symptoms appear, even if they seem mild. Prompt diagnosis allows for timely therapy, which improves outcomes. For patients and families also considering longterm survivorship and quality of life after major cancer treatments, resources on prostate cancer outlook can be useful for comparison of followup strategies and survivorship planning across cancers.
Quick Reference
RiskFactor Summary Table
| Risk Factor | Impact on Relapse Rate |
|---|---|
| inv16 cytogenetics | Up to 30% with standard-dose cytarabine |
| High WBC at diagnosis (>10010/L) | ~23 higher risk |
| Prior CNS disease | Significant increase (510%) |
| FLT3ITD mutation | Elevated risk, especially without targeted therapy |
Diagnostic Checklist
- New neurologic symptom (headache, seizure, visual change, back pain)
- Urgent MRI of brain/spine
- If MRI abnormal or symptoms persist lumbar puncture
- CSF cytology+flow cytometry for blasts
- Simultaneous blood work to rule out systemic relapse
Treatment Comparison Chart
| Approach | Efficacy (CR rate) | Key Toxicities |
|---|---|---|
| Highdose systemic cytarabine | ~70% CR in isolated CNS relapse | Cerebellar toxicity, myelosuppression |
| Intrathecal AraC+Methotrexate | ~65% CR when combined with systemic | Neuroirritation, headache, spinal pain |
| AlloHSCT after remission | 3040% 1yr OS (better than chemo alone) | GVHD, infection risk, organ toxicity |
Key Sources
For deeper dives, you can explore the NCCN AML guidelines, recent articles in Haematologica, and case reports from BMJ Case Reports. All information presented here reflects the most current peerreviewed data and expert consensus.
Conclusion
Isolated CNS relapse AML is uncommon, yet it carries serious implications if missed. Recognizing the telltale neurologic cues, acting fast with imaging and a spinal tap, and employing highdose cytarabineoften paired with intrathecal therapycan keep the disease at bay. Prevention, especially for highrisk genetic subtypes, hinges on tailored prophylaxis, and stemcell transplant offers a solid chance for durable remission.
Knowledge is power, and you dont have to walk this path alone. If youve experienced any of the symptoms described, or if you have questions about the treatment options, please share your thoughts in the comments below. Together we can turn uncertainty into confidence, one conversation at a time.
FAQs
What does isolated CNS relapse in AML mean?
It means leukemia has returned only in the central nervous system (brain, spinal cord, or cerebrospinal fluid) without evidence of disease in the bone marrow or blood.
How common is isolated CNS relapse in AML patients?
Isolated CNS relapse is uncommon, with rates generally between 1% and 8%, but can be as high as 30% in certain genetic subgroups treated with standard cytarabine.
What symptoms indicate a possible CNS relapse in AML?
Key signs include persistent headaches, blurred or double vision, seizures, facial weakness, unexplained nausea, back pain, and changes in mental status like confusion or drowsiness.
How is isolated CNS relapse diagnosed?
Diagnosis involves urgent MRI imaging followed by a lumbar puncture to analyze cerebrospinal fluid using cytology, flow cytometry, and PCR for leukemia cells or genetic mutations.
What are the main treatment options for isolated CNS relapse AML?
Treatment typically includes high-dose systemic cytarabine combined with intrathecal chemotherapy, and often allogeneic stem-cell transplantation for eligible patients.