Ever wondered why a sore knee, red eyes, and a burning pee can show up together after a stomach bug? That trio is the classic reactive arthritis triad. Its not a coincidenceyour immune system is reacting to an infection elsewhere in the body, and the inflammation can pop up in joints, eyes, and the urinary tract.
Spotting the triad early can shave weeks off your recovery, keep the pain from becoming chronic, and guide you toward the right treatment. Lets dive in, sidebyside, as if we were chatting over coffee.
What Is the Triad
In simple terms, the reactive arthritis triad consists of three main features:
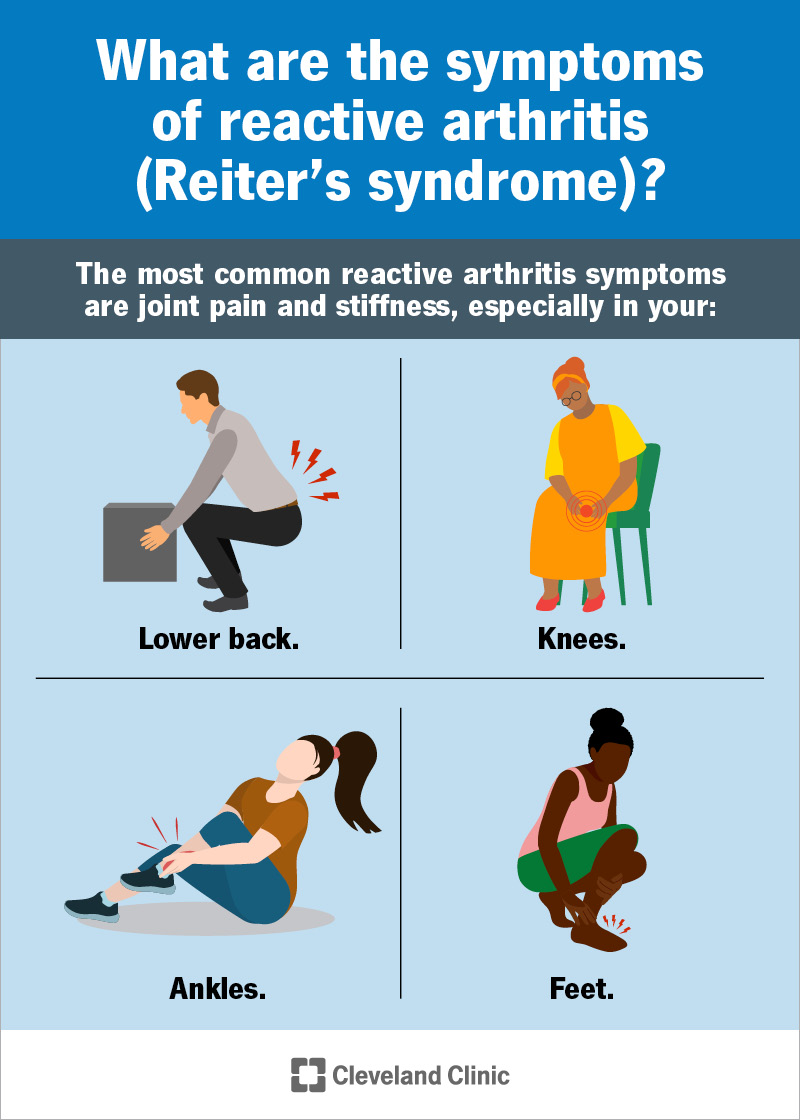
- Arthritis usually pain, swelling, and stiffness in the knees, ankles, or feet.
- Conjunctivitis redness, itching, or watery eyes (sometimes called uveitis).
- Urethritis burning or itching during urination, often accompanied by discharge.
These symptoms typically appear 14 weeks after an infection of the gastrointestinal or genitourinary tract, such as a foodborne Salmonella outbreak or a chlamydia infection. The immune system, mistaking parts of the body for the invading bugs, launches an inflammatory response that lands in these three spots.
According to , about 3050% of patients with reactive arthritis actually show the full triad; many experience only one or two components. That variability is why doctors keep a broad eye on any postinfectious joint pain.
Spotting the Triad
Imagine you just got over a bout of food poisoning. A handful of days later, your knee starts throbbing, your eyes feel gritty, and you notice a burning sensation when you pee. That patternjoint pain + eye inflammation + urinary symptomsis the hallmark that should raise a red flag.
Below is a quick comparison to help you differentiate reactive arthritis from a few lookalikes.
| Condition | Key Features | Typical Onset | Typical Triggers |
|---|---|---|---|
| Reactive Arthritis | Arthritis+Conjunctivitis+Urethritis | 14 weeks postinfection | GI/GU bacteria (Salmonella, Shigella, Chlamydia) |
| Rheumatoid Arthritis | Symmetrical joint swelling, morning stiffness | Gradual, monthsyears | Autoimmune, no infection trigger |
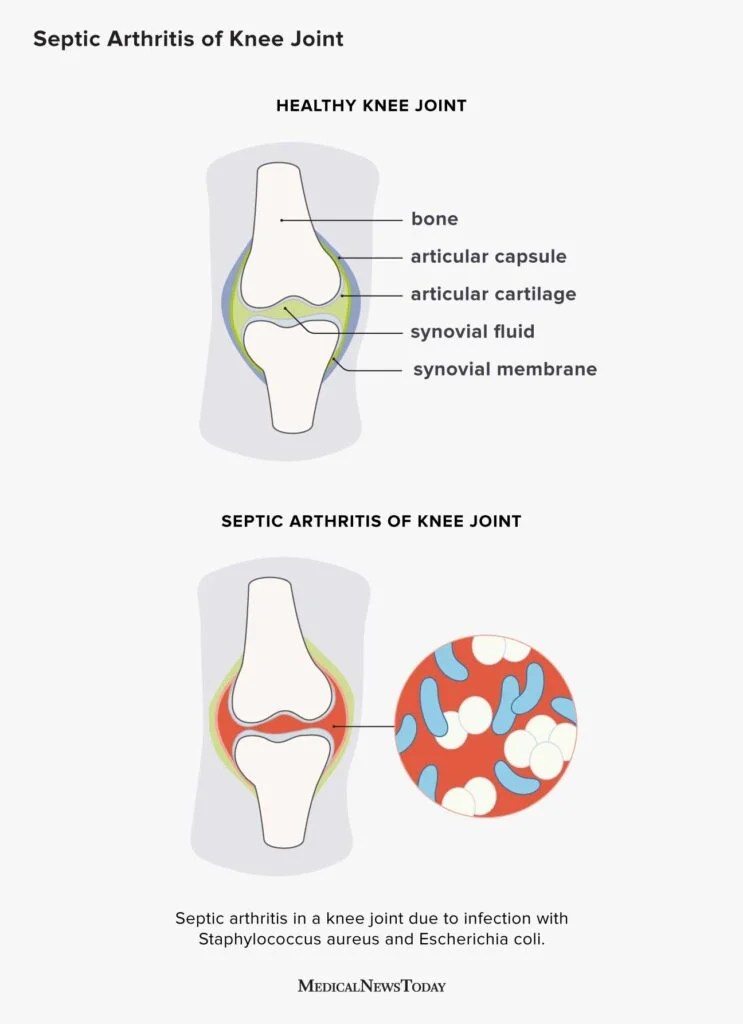
| Septic Arthritis | Severe joint pain, fever, elevated WBC | Hoursdays | Direct bacterial invasion of joint |
One anonymized case I heard about involved a 29yearold who thought his limp was just a sports injury. A few days later, he woke up with pink eyes and a painful burn every time he used the bathroom. After a quick visit to his doctor, labs confirmed the triad, and he started treatment within a weekpreventing months of lingering discomfort.
How It's Diagnosed
Diagnosis is a blend of clinical observation and targeted tests. Heres a handy checklist you can skim through:
- History of recent GI or GU infection.
- Presence of at least one component of the triad (joint pain, eye redness, urinary symptoms).
- Lab work: ESR/CRP (inflammatory markers), HLAB27 (genetic predisposition), urine culture if urethritis is suspected.
- Imaging: Xray or MRI to rule out joint damage.
Doctors also run tests to rule out mimickers. For instance, a joint tap can differentiate septic arthritis (the joint fluid looks cloudy with high neutrophils) from reactive arthritis (usually clear fluid).
Guidelines from the stress that a positive HLAB27 increases the likelihood of chronic disease, but its not required for diagnosis.
Treatment Options
Good news: many people recover fully with proper care. Treatment focuses on quelling inflammation, relieving symptoms, and preventing longterm joint damage.
Firstline: NSAIDs
Nonsteroidal antiinflammatory drugs (like ibuprofen or naproxen) are usually the start line. They tackle joint swelling, eye irritation, and the occasional lowgrade fever.
When to Add Steroids or DMARDs
If NSAIDs arent enough after a couple of weeks, a short course of oral steroids can bring relief. For persistent or recurrent cases, diseasemodifying antirheumatic drugs (DMARDs) such as sulfasalazine or methotrexate may be prescribed. A notes that DMARDs are particularly helpful when the triad lasts longer than six months.
Managing Each Piece of the Triad
- Eyes: Lubricating eye drops and, if inflammation is severe, ophthalmic steroids.
- Urethra: If a bacterial infection is still present, a short antibiotic course (often doxycycline for chlamydia) is essential.
- Joints: Physical therapy to keep the joint moving, and jointprotective exercises.
Lifestyle Support
Rest during the acute flare, balanced nutrition, and hydration help your immune system reset. Some folks find gentle yoga or swimming soothing for stiff joints, but always check with your provider first.
How Long It Lasts
Most patients see improvement within 36 months. However, about 1520% may develop chronic arthritis or recurrent eye inflammation, especially if theyre HLAB27 positive. Longterm studies show that early, aggressive treatment can cut the odds of chronic disease by roughly half.
The duration can also hinge on the original infection. For example, reactive arthritis after chlamydia often lingers a bit longer than after a foodborne bug, but both generally follow a similar course.
Triad vs Others
Its easy to confuse reactive arthritis with rheumatoid arthritis or septic arthritis, especially when joint pain dominates the picture.
- Difference between reactive arthritis and rheumatoid arthritis: RA is a chronic autoimmune disease with symmetrical joint involvement, often affecting hands and wrists first, and does not require a preceding infection.
- Reactive arthritis vs septic arthritis: Septic arthritis is a medical emergencypainful, swollen joint with fever, and the joint fluid contains live bacteria.
- Reiters syndrome triad vs reactive arthritis triad: Reiters syndrome is an older term for the same condition, emphasizing the classic triad but now less used to avoid eponym controversy.
Mnemonic & Tools
Memory can be tricky, so heres a quick mnemonic I love: ReATRIO
- Rheumatism (arthritis)
- Eye inflammation (conjunctivitis)
- After infection
- Troubles with urination (urethritis)
- Rhematic tests (HLAB27)
- Inflammatory markers (CRP/ESR)
- Optical care (eye drops)
Print it, stick it on your fridge, or download the cheatsheet PDF Ive prepared (youll find the link at the end of the article). Its handy for both patients and clinicians.
Balancing Risks & Benefits
Every medication comes with tradeoffs. NSAIDs can irritate the stomach; steroids may raise blood sugar; DMARDs have rare but serious side effects like liver toxicity. Thats why shared decisionmaking is key.
Heres a quick checklist you can discuss with your doctor:
- How severe are my symptoms?
- Do I have any medical conditions that might interact with NSAIDs or steroids?
- What is my HLAB27 status, and does it affect my longterm risk?
- Am I comfortable with a short course of antibiotics or a longer DMARD plan?
- What lifestyle changes can I make now to speed recovery?
Trusted Sources
When youre navigating health information, stick to reputable sites. Here are a few I trust and recommend:
Conclusion
The reactive arthritis triad may feel like a surprise packagejoint pain, red eyes, and a burning pee all arriving together after an infection. Knowing this pattern helps you act fast, get the right diagnosis, and start treatment before it sticks around. Early intervention, a balanced approach to medication, and lifestyle care make a huge difference, especially for those at risk of chronic disease.
If youve experienced any of these symptoms, dont waittalk to a healthcare professional. And hey, if youve got a story, a tip, or a question, drop a comment below. Sharing helps us all stay informed and supported.
For guidance on preventing recurrent joint problems and improving longterm outcomes, consider reading more about gout flare prevention as an example of lifestyle strategies that can reduce inflammatory flares across different arthritic conditions.
FAQs
What infections usually trigger the reactive arthritis triad?
The most common triggers are gastrointestinal bacteria such as Salmonella, Shigella, Campylobacter, and Yersinia, as well as the sexually transmitted bacterium Chlamydia trachomatis.
How quickly do the symptoms of the triad appear after the infection?
Symptoms typically develop 1 – 4 weeks after the initial gastrointestinal or genitourinary infection.
Is it possible for the reactive arthritis triad to become chronic?
Yes. About 15‑20 % of patients develop chronic arthritis or recurrent eye inflammation, especially if they are HLA‑B27 positive.
What laboratory and imaging tests are used to confirm reactive arthritis?
Diagnosis relies on a recent infection history, clinical signs, elevated ESR/CRP, HLA‑B27 testing, urine culture if urethritis is present, and joint X‑ray or MRI to exclude other arthritides.
How are the eye and urinary components of the triad managed?
Eye inflammation is treated with lubricating drops and, if severe, topical steroids. Urethritis is treated with appropriate antibiotics (e.g., doxycycline for chlamydia) and supportive measures.