Below youll get the straighttothepoint facts: what a chest wall tumor actually is, how to spot its warning signs, the imaging tools doctors rely on, treatment pathways, and what you can realistically expect for survival and daily life. Think of it as a friendly chat that equips you with the info you need to feel confident about the next steps.
What Is Chest Wall Tumor
Definition & Anatomy
The chest wall is the sturdy framework of ribs, sternum, intercostal muscles, and the covering pleura. When cells in any of these structures start growing out of control, a chest wall tumor forms. It can arise from bone (osteogenic), cartilage (chondrogenic), or soft tissue (muscular, fibrous). Knowing where it lives helps doctors decide which imaging test or surgical approach is best.
Primary vs. Secondary Tumors
Most adult chest wall tumors are primarythey start in the chest wall itself. However, a tumor can also be secondary (metastatic) when cancer from another organ spreads to the ribs or muscles. The distinction matters because treatment for a primary sarcoma differs from therapy for a lungcancer metastasis.
Benign vs. Malignant Types
Not every growth is dangerous. Common benign lesions include osteochondroma, chondroma, and fibrous dysplasia. Malignant typeslike chondrosarcoma, osteosarcoma, or softtissue sarcomastend to grow faster, cause pain, and may invade surrounding structures.
Benign vs. Malignant Comparison
| Feature | Benign | Malignant |
|---|---|---|
| Growth speed | Slow, often static | Rapid, often enlarges over weeks |
| Pain | Usually none or mild | Persistent, worsening pain |
| Imaging appearance | Welldefined, smooth margins | Irregular, invasive borders |
| Prognosis | Excellent after simple excision | Depends on stage; may need multimodal therapy |
Sources
For a deeper dive, see the and the .
Symptoms You Should Notice
Typical Symptoms
Most patients notice one or more of the following:
- Localized chest pain that worsens with deep breaths or movement.
- A palpable lump that may feel firm or hard.
- Restricted chest expansion, making it hard to take a full breath.
- Persistent cough or shortness of breath when the mass presses on lung tissue.
- Occasional numbness or tingling if nerves are involved.
These are the classic chest wall tumor symptoms that set off alarm bells.
FemaleSpecific Clues
Women sometimes mistake a chest wall mass for a breast issue. Tumor in chest female symptoms often include a lump near the breast that doesnt change with menstrual cycles, and pain thats not typical of mastitis. If the mass is located more laterally (toward the armpit) or superiorly (near the collarbone), think chest wall first.
When a Mass Could Be Something Else
Mass in chest what could it be? is a common question. Alternatives include lipomas (fatty benign lumps), rib fractures with callus formation, infections like abscesses, or even enlarged lymph nodes. A thorough exam and imaging will narrow it down.
Quick Symptom Checklist
Print this out or keep it on your phone:
- Is the lump hard?
- Does it hurt when you breathe?
- Is it growing over weeks?
- Any new shortness of breath?
- Any recent chest radiation?
If you tick three or more, schedule a medical appointment.
Who Is At Risk
Age & Gender Trends
Chest wall tumors can appear at any age, but the median diagnosis age is around 4555years. Men are slightly more likely to develop malignant sarcomas, yet women often present later because they may attribute the lump to breast tissue.
Risk Factors
Key factors that raise the odds:
- Prior radiation therapy to the chest (e.g., for lymphoma).
- Chronic inflammatory diseases such as ankylosing spondylitis.
- Inherited cancerpredisposition syndromes (LiFraumeni, hereditary retinoblastoma).
- Heavy occupational exposure to asbestos or certain chemicals.
RiskFactor Matrix
| Factor | Benign Risk | Malignant Risk |
|---|---|---|
| Radiation history | Low | High |
| Genetic syndrome | Low | Very High |
| Age >50 | Moderate | Moderate |
| Occupational exposure | Low | Elevated |
How Is It Diagnosed
FirstLine Evaluation
It starts with a detailed history and a physical exam. Your doctor will note the size, consistency, and mobility of the lump, as well as any associated pain or breathing difficulty.
Chest Wall Tumor Radiology
Imaging is the real gamechanger. Heres the usual ladder:
- Chest Xray: Quick, cheap, shows bone involvement.
- CT scan: Provides crosssectional views, highlights calcifications and exact location.
- MRI: Best for softtissue detail and spinal involvement.
- PETCT: Detects metabolic activity; crucial for staging and spotting metastases.
- Bone scan: Useful if you suspect osteogenic lesions.
Seeing chest wall tumor pictures on reputable sites can help you understand what radiologists are looking for, but rememberonly a trained professional can read them accurately.
Biopsy Techniques
Imaging alone cant tell you if a tumor is benign or malignant. A tissue sample is required. Options include:
- Coreneedle biopsy (imageguided, outpatient).
- Fineneedle aspiration (small sample, quicker).
- Open surgical biopsy (reserved for hardtoreach lesions).
Pathology reports will describe the cell type, grade, and any molecular markers that guide therapy.
Sources
Guidelines from the and the diagnostic algorithm outlined by are excellent references.
Treatment Options Overview
Surgical Resection
When the tumor is operable, surgery aims for a clean marginremoving the tumor plus a rim of healthy tissue. Reconstruction may involve muscle flaps, synthetic meshes, or even 3Dprinted ribs to restore chest stability.
Radiation Therapy
Radiation can be used before surgery (neoadjuvant) to shrink the tumor, or after (adjuvant) to kill residual cells. Modern techniques like IMRT or proton therapy focus the dose while sparing heart and lungs.
Chemotherapy & Targeted Agents
For highgrade sarcomas, multidrug regimens (e.g., doxorubicin + ifosfamide) are standard. Some tumors express specific mutations, opening the door to targeted therapiesthough research is still evolving.
Multidisciplinary Care
Best outcomes come from a team: thoracic surgeon, medical oncologist, radiation oncologist, radiologist, and physiatrist. Together they craft a plan that balances tumor control with quality of life.
Recovery Timeline
| Phase | Typical Duration | Key Activities |
|---|---|---|
| Hospital stay | 37 days | Pain control, early ambulation |
| Wound healing | 24 weeks | Incision care, light stretching |
| Respiratory rehab | 46 weeks | Breathing exercises, physiotherapy |
| Return to work | 612 weeks | Gradual workload increase |
Sources
Clinical pathways described by the and the treatment algorithms from the are reliable references.
Prognosis And Survival
Chest Wall Cancer Life Expectancy
Life expectancy varies dramatically. For lowgrade, completely resected sarcomas, many patients enjoy a normal lifespan. Highgrade or metastatic disease shortens median survival to 24 years, but newer systemic therapies are nudging those numbers upward.
Chest Wall Tumor Survival Rate
According to SEER data, the 5year survival rate for all chest wall sarcomas hovers around 55%. Benign lesions have a virtually 100% survival after simple excision. Early detection and a clear surgical margin are the biggest influencers.
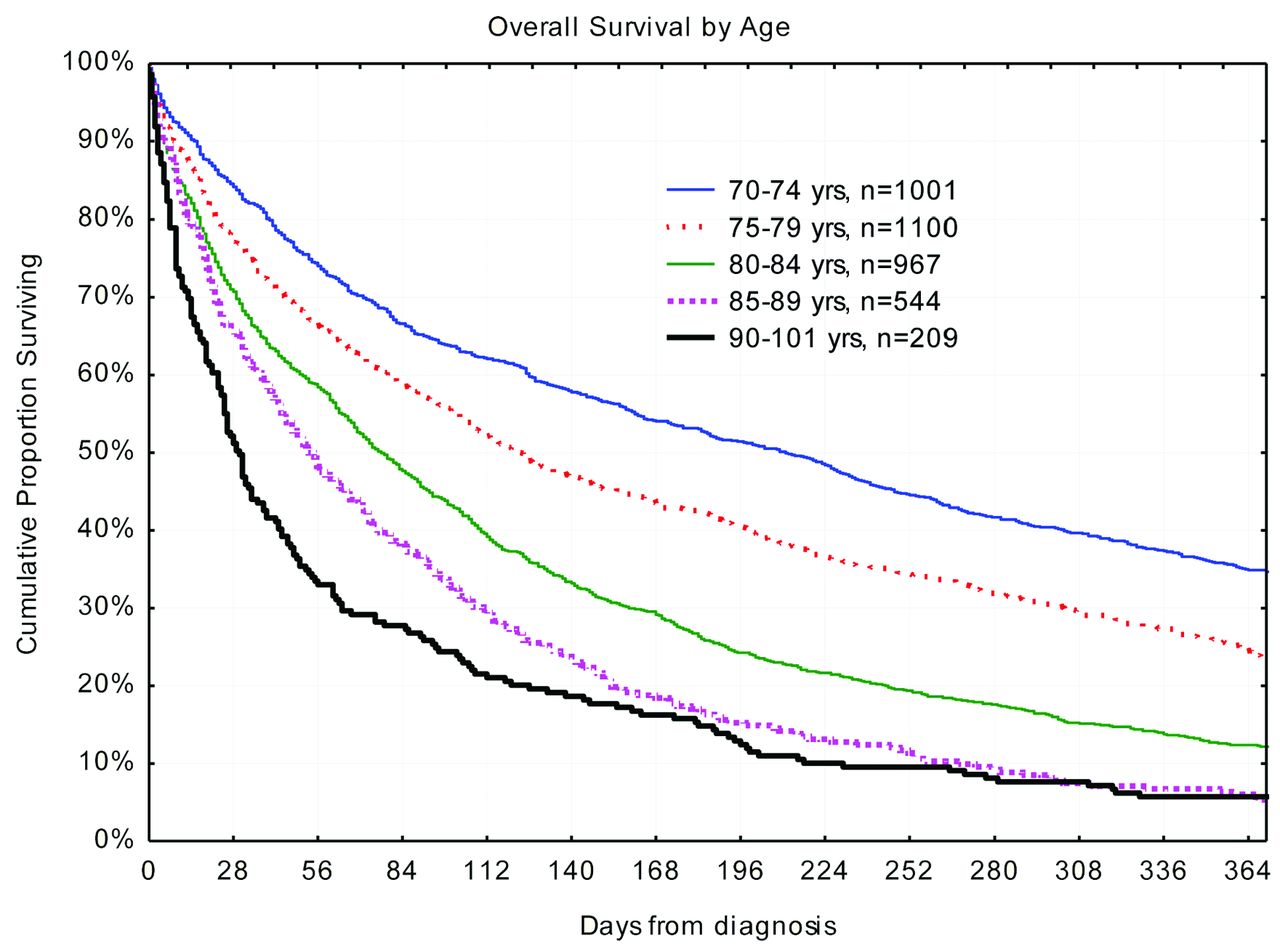
Survival Trend Graph
| Year | 5Year Survival % |
|---|---|
| 2000 | 48 |
| 2005 | 51 |
| 2010 | 54 |
| 2015 | 56 |
| 2020 | 58 |
These modest gains reflect better imaging, refined surgical techniques, and more effective adjuvant therapies.
Living After Diagnosis
PostTreatment Monitoring
Followup usually involves:
- CT or MRI every 36 months for the first two years.
- Annual scans thereafter, unless new symptoms appear.
- Blood work if youre on targeted drugs.
Keeping a symptom diary helps your team spot recurrences early.
Managing Pain & Breathing
Persistent chest pain isnt uncommon. A pain specialist may use nerve blocks or lowdose opioids. Breathing exerciseslike diaphragmatic breathing and incentive spirometryimprove lung capacity and reduce scar tissue stiffness.
Emotional & Social Support
A cancer diagnosis shakes more than just your body. Connecting with support groups (e.g., American Cancer Society forums) and seeking counseling can buffer anxiety and depression. Remember, youre not alone.
Helpful Resources
Reliable information can be found at the , the , and patientrun chest wall tumor communities.
Conclusion
Understanding a chest wall tumorfrom what it is, how it feels, and how doctors pin it downgives you power over an unsettling situation. Early recognition of symptoms, prompt imaging, and a coordinated treatment plan can dramatically improve survival and quality of life. If you or a loved one notice a persistent lump or new chest discomfort, dont waittalk to a healthcare professional, get the right scans, and start the conversation about next steps. For patients also managing cancer risks in other organs, checking resources on colon cancer genetic testing may be useful when considering hereditary syndromes that affect treatment and surveillance strategies. Feel free to share your questions or experiences in the comments below; were all in this together, and your story might just help someone else take that first brave step.
FAQs
What are the common symptoms of a chest wall tumor?
Typical signs include localized chest pain that worsens with breathing or movement, a firm palpable lump, limited chest expansion, persistent cough or shortness of breath, and occasional numbness or tingling if nerves are involved.
How are chest wall tumors diagnosed?
Diagnosis starts with a detailed history and physical exam, followed by imaging such as X‑ray, CT, MRI, and PET‑CT. A definitive diagnosis requires a tissue sample obtained by core‑needle, fine‑needle aspiration, or open biopsy.
What treatment options are available for malignant chest wall tumors?
Management usually involves surgical resection with clear margins, often combined with radiation therapy (pre‑ or post‑operative) and multi‑drug chemotherapy. Targeted therapies may be considered for tumors with specific molecular markers.
What factors affect the prognosis and survival rates?
Key prognostic factors include tumor grade, size, location, completeness of surgical removal, presence of metastasis, and patient age. Low‑grade, fully resected sarcomas have the best outcomes, while high‑grade or metastatic disease lowers 5‑year survival to around 55 %.
How often should follow‑up imaging be done after treatment?
Most guidelines recommend CT or MRI every 3–6 months for the first two years, then annually thereafter, or sooner if new symptoms develop.