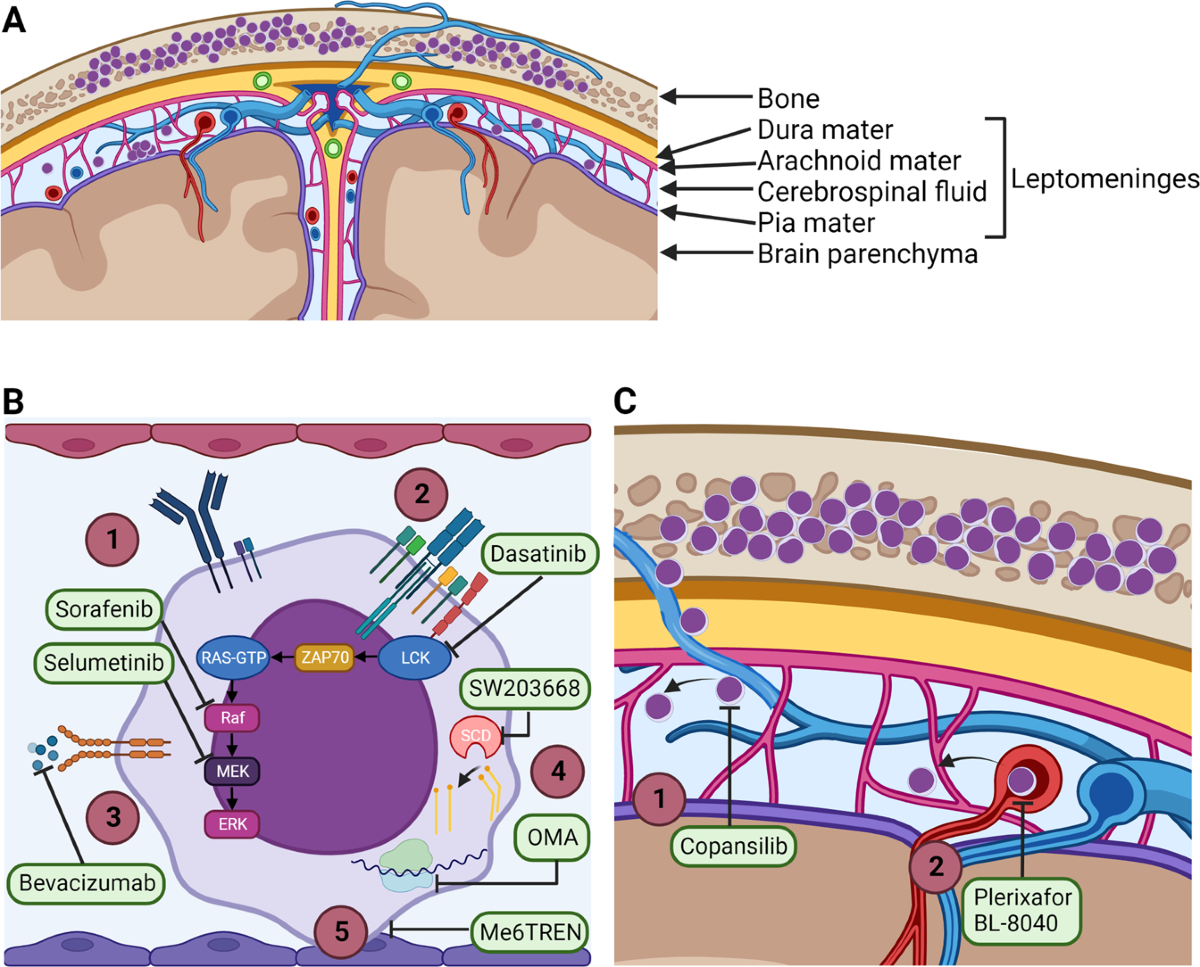
If leukemic cells have sneaked into the cerebrospinal fluid (CSF), it means the disease has taken a detour into the central nervous system (CNS). This can shift the whole treatment plan, change survival numbers, and bring a whole new set of symptoms you might not have expected.
Getting clear, actionable information right now can make a big differencewhether youre a patient, a parent, or just trying to understand what the doctor meant when they mentioned CNS involvement. In the next few minutes well walk through what it looks like, how its diagnosed, how the numbers stack up, and what treatments are actually helping people today.
What Is CNS Leukemia
What does leukemia in CSF actually mean?
Leukemia originates in the bonemarrow, but the malignant cells can travel through the bloodstream and end up in the CSF, the clear fluid that bathes the brain and spinal cord. When that happens, doctors call it CNS leukemia or leukemia in CSF. Its a sign that the disease has found a sanctuary where many chemotherapy drugs struggle to reach.
How common is CNS involvement?
Its relatively rare but not negligible. Roughly 4% of children with acute lymphoblastic leukemia (ALL) and up to 15% of adults with acute myeloid leukemia (AML) have detectable blasts in the CSF at diagnosis or during treatment .
Why does leukemia spread to the spinal fluid?
The CSF provides a protective nichecalled a biological sanctuarywhere leukemic cells can hide from systemic therapy. The bloodbrain barrier limits drug penetration, so if any cells slip in early, they can expand unchecked.
Quick data snapshot
| Age Group | Leukemia Type | CSF Involvement Rate |
|---|---|---|
| Children (ALL) | Acute Lymphoblastic | 4% |
| Adults (AML) | Acute Myeloid | 1015% |
Detecting Leukemia in CSF
Which tests are used?
The goldstandard is a lumbar puncture, where a small amount of CSF is drawn and examined. Cytology looks for obvious blast cells under a microscope, while flow cytometry can detect even a tiny fraction of leukemic cells. Molecular PCR tests are also emerging as ultrasensitive tools.
What does a count of 5 leukocytes/L mean?
Studies show that when the total nucleated cell (TNC) count climbs above 5cells/L, about half the patients start showing neurologic symptoms. Below that threshold, up to 80% remain asymptomatic, though the disease may still be present.
Can CSF biomarkers predict relapse?
Yes. Certain markerslike elevated CD19+ blasts detected by flow cytometrycorrelate with a higher risk of CNS relapse. Ongoing research is refining these predictive models .
Test comparison
| Method | Sensitivity | Cost | Turnaround |
|---|---|---|---|
| Cytology | ~60% | Low | 12days |
| Flow Cytometry | ~90% | Medium | 23days |
| PCR (Molecular) | >95% | High | 12weeks |
Symptoms of Spinal Fluid Involvement
What are the most common neurologic signs?
Headaches, especially worse in the morning, blurry vision, nausea, and occasional vomiting are classic. Some patients also experience gait disturbances, back pain, or facial weakness if the disease presses on cranial nerves.
Can patients be completely asymptomatic?
Absolutely. Many people with lowlevel CSF disease feel perfectly fine, which is why routine CSF checks are crucial in highrisk groups.
How do symptoms differ between kids and adults?
Kids often present with irritability, changes in behavior, or unexplained vomiting, whereas adults may first notice visual changes or severe headaches. The underlying biology is similar; its the way we express discomfort that varies.
Realworld anecdote
Take eightyearold Maya, who was diagnosed with ALL. She started having frequent headaches and occasional double vision. A quick lumbar puncture revealed blasts in her CSF, prompting an immediate shift to intrathecal therapy. Within a month, her symptoms faded, and her oncologist called it a win for early detection.
Survival Rates & Prognosis
What is the overall survival outlook?
When leukemia spreads to the CSF, fiveyear overall survival drops compared to CNSnegative cases. In ALL, CNSpositive patients have roughly a 75% fiveyear survival versus 90% for those with no CNS disease. In AML, the gap is largerabout a 45% survival for CNSpositive versus 6070% for CNSnegative.
How does leukemia in spinal fluid survival rate differ by type?
ALL tends to respond better to intrathecal methotrexate, so the prognosis improves significantly once CNS therapy starts. AML, on the other hand, is less sensitive to standard intrathecal drugs, which reflects the generally lower survival rates.
Key prognostic factors
- Blast count in CSF (higher counts poorer outlook)
- Age (younger children often fare better)
- Genetic mutations (e.g., Philadelphia chromosome)
- Response to initial CNSdirected therapy
Infographic sketch (for the full article)
Imagine a sidebyside bar chart: CNSNegative vs. CNSPositive for ALL and AML, showing the 5year OS percentages mentioned above. Visuals help the numbers stick.
Treatment Options for CNSPositive Leukemia
Does highdose systemic chemotherapy reach the CSF?
Some agentslike highdose cytarabinepenetrate the CSF somewhat, but theyre rarely enough on their own. Thats why dedicated CNS therapy is standard.
Whats intrathecal chemotherapy?
Doctors inject drugs directly into the CSF via a lumbar puncture. The usual cocktail includes methotrexate, cytarabine, and a steroid like dexamethasone. Doses are given weekly at first, then spaced out depending on response.
Can newer targeted therapies cross the bloodbrain barrier?
Yes! Blinatumomab (a BiTE antibody) and some CART cell products have shown activity in the CNS. Early trials suggest they can clear blasts that survive intrathecal regimens, though longterm data are still rolling in.
When is radiation therapy needed?
Radiation is reserved for refractory cases or when CNS disease is extensive. Because of the risk of cognitive declineespecially in childrendoctors try to limit its use.
Stepbystep 12week protocol (example)
- Weeks14: Twiceweekly intrathecal methotrexate + dexamethasone.
- Weeks58: Add weekly cytarabine intrathecally.
- Weeks912: Consolidation with highdose systemic methotrexate + intrathecal maintenance every 2weeks.
Sideeffect checklist
- Meningeal irritation (neck stiffness, fever)
- Neurotoxicity (temporary confusion, seizures)
- Longterm cognitive effects (more common with radiation)
Special Considerations for Children
Why are kids more prone to CNS involvement?
Childrens bloodbrain barriers are slightly more permissive, and the rapid proliferation of leukemic blasts in pediatric ALL often targets the CNS early.
How does dosing differ for pediatric patients?
Intrathecal doses are weightadjusted and often administered more frequently to keep the disease in check. Pediatric oncologists also monitor growth and neurodevelopment closely during treatment.
What about longterm survivorship?
Even after successful eradication, survivors can face challenges like learning difficulties, reduced memory capacity, or subtle motor delays. Early intervention programs and regular neurocognitive testing are vital.
Case series summary
A cohort of 50 pediatric ALL patients with CNS2 (lowlevel blasts) versus CNS3 (highlevel blasts) showed a 5year eventfree survival of 88% versus 72% respectively, underscoring the importance of early, aggressive CNS therapy .
Monitoring & FollowUp
How often should CSF be resampled?
During induction, lumbar punctures are typically performed twice a week until CSF clears, then weekly for several weeks, and finally monthly during consolidation. After therapy, most centers do a check at 3, 6, 12, and 24months.
What lab thresholds trigger a treatment change?
If blasts reappear or the TNC count climbs above 5cells/L on two consecutive samples, physicians usually intensify intrathecal therapy or add systemic agents that penetrate the CNS.
Is MRI ever needed?
Yesespecially when patients develop focal neurologic deficits. MRI can reveal leptomeningeal enhancement or spinal cord compression that a lumbar puncture alone might miss.
Posttherapy surveillance checklist
- CSF analysis at months0,3,6,12,24.
- Annual MRI if any prior CNS symptoms.
- Neurocognitive assessment every 23years for children.
- Prompt reporting of new headaches, visual changes, or gait disturbances.
Key Takeaways
Leukemia that reaches the CSF is a serious, but increasingly manageable, complication. Early detection through routine lumbar punctures, combined with modern intrathecal chemotherapy and emerging targeted therapies, can dramatically improve survivalespecially for children with ALL. However, the journey isnt just about numbers; its about watching out for subtle symptoms, staying vigilant with followup, and leaning on a care team that balances aggressive treatment with qualityoflife considerations.
If you or a loved one are navigating this road, talk openly with your oncologist about CSF monitoring schedules, ask about the newest CNSpenetrating drugs, and dont shy away from asking for a neurocognitive evaluation if youre a parent. Knowledge and proactive care are your strongest allies.
What experiences have you or someone you know had with CNS leukemia? Share your story in the comments or reach out with questionsyoure not alone in this.
FAQs
What does a positive “leukemia in CSF” result indicate?
A positive result means leukemic blast cells have been found in the cerebrospinal fluid, confirming central‑nervous‑system involvement and prompting CNS‑directed therapy.
How is leukemia in CSF diagnosed?
Diagnosis is made by lumbar puncture. The collected CSF is examined with cytology, flow cytometry, and increasingly with PCR‑based molecular tests to detect even minimal disease.
What are the most common symptoms of CNS leukemia?
Typical signs include persistent morning headaches, nausea or vomiting, blurry vision, gait disturbances, and, in children, irritability or unexplained vomiting.
Which treatment options are used for leukemia in CSF?
Standard care involves intrathecal chemotherapy (methotrexate, cytarabine, dexamethasone), high‑dose systemic agents that cross the blood‑brain barrier, and, when needed, targeted therapies such as blinatumomab or CAR‑T cells. Radiation is reserved for refractory disease.
How often should CSF be checked after completing therapy?
After remission, CSF is usually sampled at the end of treatment, then at 3, 6, 12 and 24 months. Ongoing surveillance may be performed annually or sooner if new neurological symptoms appear.