If a child receives a diagnosis of a softtissue sarcoma, the news can feel like a sudden storm. In the next few minutes youll get straighttothepoint factswhat the disease is, what it looks like, how doctors figure it out, the treatment choices, and what the numbers say about survivalso you can ask the right questions and feel a little more in control.
Understanding the Disease
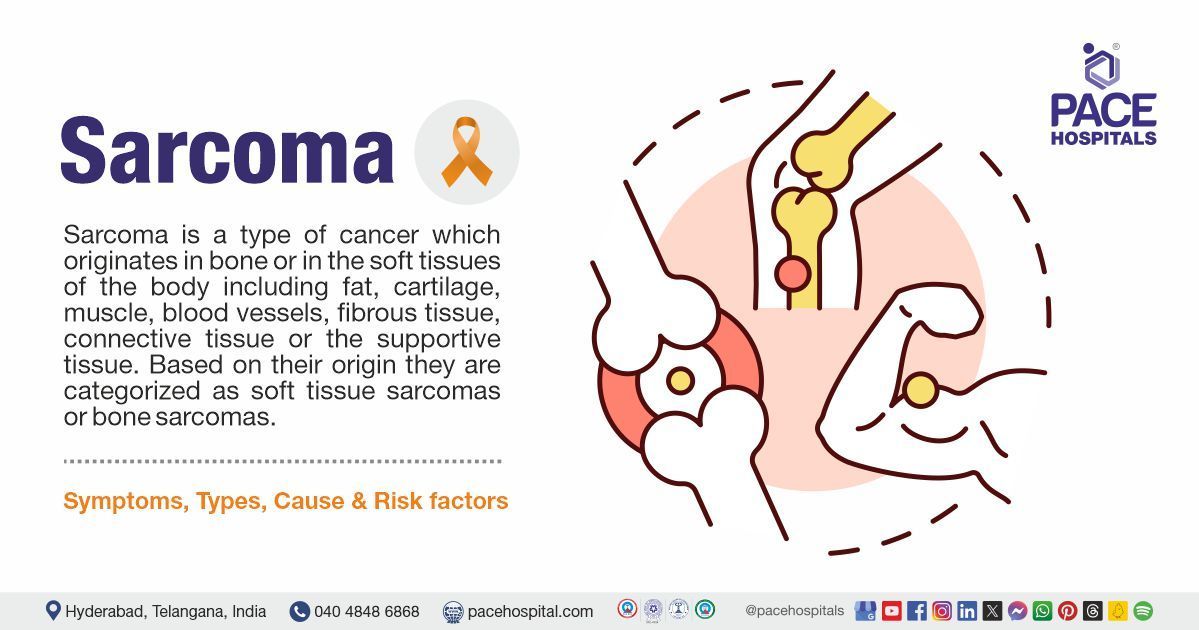
What does softtissue sarcoma mean?
In simple terms, a softtissue sarcoma is a cancer that starts in the bodys connective tissuesmuscle, fat, nerves, blood vessels, or the lining that holds everything together. When this happens in a child, we add the word pediatric to remind us that kids arent just small adults; their bodies grow, and their cancers often behave differently.
How common is it?
Softtissue sarcomas account for roughly 7% of all childhood cancers, translating to about 850900 new cases of rhabdomyosarcoma (the most frequent type) each year in the United States. While the odds of a child developing any sarcoma are low, the rarity makes it crucial to spot early signs and get expert care.
Key Statistics
| Age Group | Incidence (per 1M) | Most Common Type |
|---|---|---|
| 04 years | 2.3 | Rhabdomyosarcoma |
| 59 years | 1.8 | Rhabdomyosarcoma |
| 1014 years | 1.2 | Ewing Sarcoma |
Why does softtissue matter?
The term signals that the tumor arises outside of bone. This matters because treatment pathways (surgery, radiation, chemotherapy) differ from those used for bone cancers, and the prognosis often hinges on how easily the tumor can be removed. For some sarcoma types, early prostate cancer in adults offers a contrasting example, where early detection dramatically shapes outcomes and treatment options in both adult and pediatric cancers.
Common Types & Benign
Rhabdomyosarcoma the most common malignant type
Rhabdomyosarcoma (RMS) is a cancer that mimics developing skeletal muscle. It comes in several subtypes:
- Embryonal most frequent in younger children, usually in the head, neck, or genitals.
- Alveolar tends to affect older kids and can spread more aggressively.
- Pleomorphic rare, seen in teenagers.
Subtype Comparison
| Subtype | Typical Age | Common Sites | 5Year Survival |
|---|---|---|---|
| Embryonal | 28 years | Head/neck, genitals | 75% |
| Alveolar | 1015 years | Extremities, trunk | 55% |
| Pleomorphic | Teenagers | Extremities | 45% |
Other malignant softtissue sarcomas
Beyond RMS, children can develop:
- Ewing sarcoma often starts in bone but can arise in soft tissue.
- Synovial sarcoma typically seen near joints.
- Infantile fibrosarcoma appears in babies, usually curable with surgery.
Most common benign softtissue tumor in childhood
While we focus on cancer, its worth noting that the most frequent benign counterpart is the infantile hemangioma, a harmless vascular growth that often fades on its own. Lipomas (fatty lumps) and fibromatoses also pop up but rarely cause trouble.
Signs & Symptoms
Early red flags
Parents often notice a painless lump or swelling that doesnt go away. Other clues include:
- Unexplained pain that worsens with movement.
- Reduced range of motion in a limb.
- Visible bulge under the skin that grows over weeks.
- Unusual bruising or skin changes over a mass.
Locationspecific clues
A lump in the neck or head may cause trouble swallowing or breathing. Tumors in the abdomen can lead to a feeling of fullness or early satiety. When the tumor presses on nerves, you might see tingling or weakness in the affected area.
Quick SoftTissue Sarcoma in Child Symptoms Checklist
- Painless, firm lump that enlarges.
- Persistent pain or tenderness.
- Limited movement of a nearby joint.
- Unexplained swelling or bruising.
- Changes in skin texture over the area.
What happens if its ignored?
Delays in diagnosis can allow the tumor to grow larger, making surgery more complex and sometimes lowering survival chances. In rare cases when soft tissue cancer spreads to organs like the kidney, Kidney cancer diet may become relevant for supportive care during treatment.
Diagnosis and Pathology
Imaging tools
Doctors usually start with an ultrasound to see if the lump is solid. If it looks suspicious, an MRI gives a detailed map of the tumors size and relationship to muscles, nerves, and blood vessels. In some cases, a CT scan or PET scan helps to check whether the cancer has spread.
Biopsy techniques
The definitive answer comes from a tissue sample. A core needle biopsy removes a small cylinder of tissue, while an excisional biopsy takes the whole lump out. The choice depends on the tumors location and size.
Pediatric soft tissue tumors pathology
Under the microscope, pathologists look for specific patterns. RMS, for example, shows cells that try to look like developing muscle fibers. They also run immunohistochemistry stainsspecial dyes that highlight proteins unique to each cancer type. Molecular testing can reveal gene fusions such as FOXO1, which is typical for alveolar RMS.
Why pathology matters
Accurate classification tells the treatment team whether the tumor is likely to respond to standard chemotherapy or whether newer targeted drugs might be an option.
Treatment Options Overview
Surgery
When the tumor is localized, surgeons aim to remove it completely while preserving as much function as possible. Limbsparing techniques and robotic assistance have made it easier to keep kids active after surgery.
Radiation therapy
Radiation can shrink tumors before surgery (neoadjuvant) or clean up leftover cells afterward (adjuvant). Modern techniques like intensitymodulated radiation therapy (IMRT) focus the beam tightly to protect surrounding healthy tissue.
Chemotherapy regimens
The classic VAC comboVincristine, ActinomycinD, and Cyclophosphamideis the backbone of most pediatric soft tissue sarcoma protocols. Its given in cycles every few weeks, and while the side effects (nausea, hair loss, low blood counts) are tough, theyre carefully monitored.
Targeted and immunotherapy
For tumors with specific genetic changes, drugs that home in on those alterations are now entering clinical trials. Immunotherapy, which teaches the immune system to attack cancer cells, is also being explored, especially for relapsed disease.
Finding a trial
If youre looking for cuttingedge options, clinical trials listed on ClinicalTrials.gov often filter by pediatric soft tissue sarcoma and can connect you with specialized centers. For individuals or families also seeking diet support during or after cancer, learning about a Cancer diet plan may be helpful as part of holistic recovery and strength maintenance.
Survival Rates Overview
Overall pediatric sarcoma survival rate
According to the National Cancer Institute, children with localized RMS have a fiveyear survival of about 70%. If the disease has spread (metastatic), the rate drops to roughly 3040%.
Factors that influence outcome
- Age at diagnosis younger children sometimes have better responses.
- Tumor size smaller tumors are easier to remove fully.
- Location tumors in the head and neck can be tricky because of nearby critical structures.
- Histology embryonal RMS generally does better than alveolar.
- Response to initial therapy tumors that shrink quickly with chemotherapy have a better prognosis.
Survival Comparison Table
| Condition | 5Year Survival (Localized) | 5Year Survival (Metastatic) |
|---|---|---|
| Embryonal RMS | 80% | 45% |
| Alveolar RMS | 60% | 30% |
| Other SoftTissue Sarcoma | 70% | 35% |
What survival rate really means
A survival rate isnt a personal prediction; its an average for groups of patients treated similarly. Individual outcomes can differ widely based on the factors above and the quality of the care team.
Helpful Resources Guide
Trusted organizations
Reputable groups can give you uptodate information and emotional support:
- National Cancer Institute according to the NCI
- St.Jude Childrens Research Hospital
- CureSearch for Children with Cancer
- Childrens Hospital of Philadelphia Sarcoma Program
Tools you might find handy
- Symptomtracker apps (e.g., CareClinic) to log pain, swelling, and medication side effects.
- Geneticcounseling checklists for families planning future pregnancies.
- Appointment preparation sheet bring a list of questions, current meds, and a copy of the pathology report.
Preparing for the first oncology visit
Walking into a pediatric oncology clinic can feel daunting. Heres a quick checklist to make it smoother:
- Write down the childs full medical history (including any previous surgeries).
- Note all current medications, supplements, and allergies.
- Prepare a list of questions: What is the exact type of sarcoma?, What are the shortterm side effects?, How often will we need imaging?
- Bring a trusted adult or friend for supportyou shouldnt have to remember everything alone.
Conclusion
Pediatric soft tissue sarcoma may sound frightening, but understanding the diseaseits types, warning signs, how its diagnosed, and the range of treatmentsgives families a solid footing to ask the right questions and partner with their care team. Survival rates have improved dramatically thanks to surgery, modern chemotherapy, and emerging targeted therapies, especially when the cancer is caught early. Use the resources above to stay informed, connect with specialists, and find community support. If you or someone you love is facing a diagnosis, reach out to a pediatric oncology center today; the sooner you act, the better the chances of a positive outcome.
FAQs
What is pediatric soft tissue sarcoma?
It is a rare cancer that begins in the connective tissues (muscle, fat, nerves, blood vessels) of children, behaving differently from adult sarcomas.
Which type of soft‑tissue sarcoma is most common in children?
Rhabdomyosarcoma (RMS) is the most frequent malignant soft‑tissue sarcoma in the pediatric population.
What are the early warning signs parents should watch for?
Painless, firm lumps that grow, persistent pain, limited joint movement, unexplained swelling or bruising, and skin changes over a mass.
How is a pediatric soft tissue sarcoma diagnosed?
Diagnosis begins with imaging (ultrasound, MRI, CT/PET) followed by a tissue biopsy—core needle or excisional—to confirm the tumor type.
What treatment options are available for children with localized disease?
Standard care includes surgery to remove the tumor, often combined with chemotherapy (VAC regimen) and radiation therapy; targeted therapies are emerging for specific genetic sub‑types.