But its not just about raising the count. You also need to understand why cirrhosis drags your platelets down, weigh the benefits against the risks of each treatment, and work with a liverfriendly team that tailors a plan just for you. In the next few minutes well walk through the science, the options, and a simple checklist you can use the next time you talk to your doctor.
Understanding the Problem
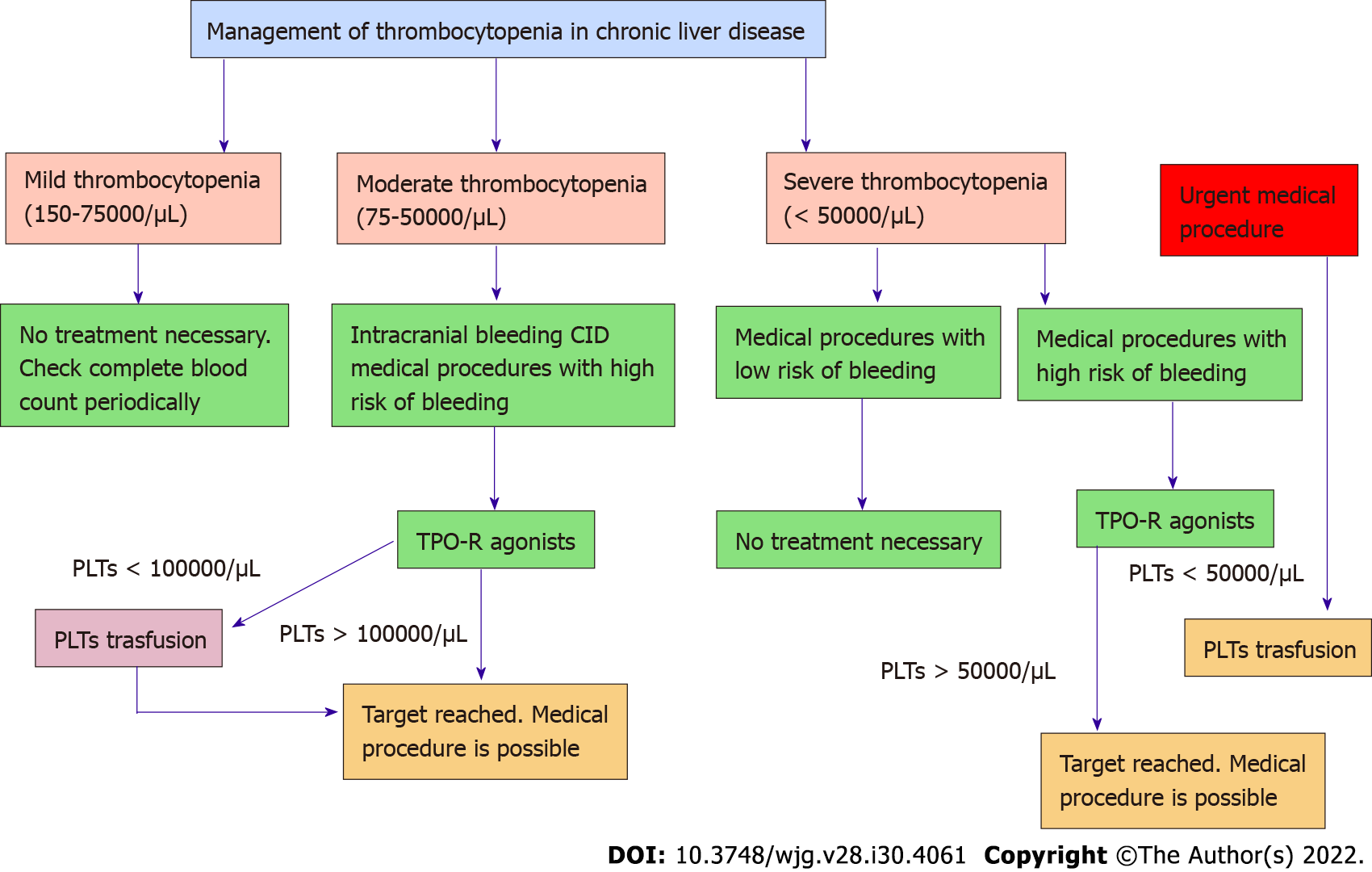
First, lets clear up what thrombocytopenia in cirrhosis actually means. A normal platelet count for a healthy adult sits between 15010/L and 45010/L. In people with advanced liver disease, those numbers can dip well below 10010/L, and in severe cases they may fall under 5010/L. This drop isnt random; its a direct consequence of the livers diminished ability to make thrombopoietin (the hormone that tells the bone marrow to produce platelets) and the high pressure in the portal vein that causes the spleen to trap more platelets than it should.
Why does cirrhosis cause low platelets? Two main mechanisms drive the process:
- Portal hypertension. As scar tissue blocks blood flow through the liver, pressure builds up in the portal system. The spleen expands (splenomegaly) and starts hoarding platelets, removing them from circulation.
- Reduced thrombopoietin production. A diseased liver cant crank out enough of this key hormone, so the bone marrow gets fewer orders to churn out new platelets.
When should you start worrying? Generally, a platelet count under 10010/L prompts closer monitoring, especially if you need an invasive procedure like a liver biopsy or endoscopy. Below 5010/L, the risk of spontaneous bleeding rises and most physicians will consider active treatment.
| Platelet Count | Typical Concern | Action Needed |
|---|---|---|
| >15010/L | Normal | No specific treatment |
| 10015010/L | Minor procedures | Monitor |
| 5010010/L | Endoscopy, biopsy | Consider treatment |
| <5010/L | Highrisk surgery | Treat (see options below) |
Proven Treatments
Now that we know when to act, lets explore the toolbox. Each option has its own set of pros, cons, and suitability factors.
Platelet Transfusion The Quick Fix
If youre about to undergo an urgent procedure, a transfusion can raise your platelet count by 305010/L within a few hours. Its effective, but the boost is shortlived (usually 4872hours) and repeated transfusions can lead to alloimmunizationyour body developing antibodies that make future transfusions less effective. Because of these risks, doctors reserve transf
But its not just about raising the count. You also need to understand why cirrhosis drags your platelets down, weigh the benefits against the risks of each treatment, and work with a liverfriendly team that tailors a plan just for you. In the next few minutes well walk through the science, the options, and a simple checklist you can use the next time you talk to your doctor.
Understanding the Problem
First, lets clear up what thrombocytopenia in cirrhosis actually means. A normal platelet count for a healthy adult sits between 15010/L and 45010/L. In people with advanced liver disease, those numbers can dip well below 10010/L, and in severe cases they may fall under 5010/L. This drop isnt random; its a direct consequence of the livers diminished ability to make thrombopoietin (the hormone that tells the bone marrow to produce platelets) and the high pressure in the portal vein that causes the spleen to trap more platelets than it should.
Why does cirrhosis cause low platelets? Two main mechanisms drive the process:
- Portal hypertension. As scar tissue blocks blood flow through the liver, pressure builds up in the portal system. The spleen expands (splenomegaly) and starts hoarding platelets, removing them from circulation.
- Reduced thrombopoietin production. A diseased liver cant crank out enough of this key hormone, so the bone marrow gets fewer orders to churn out new platelets.
When should you start worrying? Generally, a platelet count under 10010/L prompts closer monitoring, especially if you need an invasive procedure like a liver biopsy or endoscopy. Below 5010/L, the risk of spontaneous bleeding rises and most physicians will consider active treatment.
| Platelet Count | Typical Concern | Action Needed |
|---|---|---|
| >15010/L | Normal | No specific treatment |
| 10015010/L | Minor procedures | Monitor |
| 5010010/L | Endoscopy, biopsy | Consider treatment |
| <5010/L | Highrisk surgery | Treat (see options below) |
Proven Treatments
Now that we know when to act, lets explore the toolbox. Each option has its own set of pros, cons, and suitability factors.
Platelet Transfusion The Quick Fix
If youre about to undergo an urgent procedure, a transfusion can raise your platelet count by 305010/L within a few hours. Its effective, but the boost is shortlived (usually 4872hours) and repeated transfusions can lead to alloimmunizationyour body developing antibodies that make future transfusions less effective. Because of these risks, doctors reserve transfusions for highrisk surgeries or when other options arent feasible.
Thrombopoietin Receptor Agonists (TPORAs)
These oral or injectable medications trick the bone marrow into making more platelets, essentially substituting the missing thrombopoietin signal.
- Avatrombopag and Lusutrombopag have gained FDA approval specifically for chronic liver diseaserelated thrombocytopenia. In a pivotal phaseIII trial, patients receiving lusutrombopag achieved a platelet count 5010/L in 80% of cases, enough to safely undergo elective procedures.
- Eltrombopag is used offlabel; a showed a mean increase of 3010/L after 6 weeks in HCVrelated cirrhosis.
When prescribing TPORAs, clinicians watch for potential side effects like thrombosis (especially in patients with a history of blood clots) and liver enzyme elevations. The good news is that the rise in platelets tends to be gradual and can be sustained long enough to cover a scheduled procedure.
Partial Splenic Embolization (PSE)
This minimally invasive radiology technique blocks part of the splenic artery, reducing the spleens ability to trap platelets. Most patients see a 306010/L increase within a month, and the improvement can last for years. The main drawbacks are postembolization fever, pain, and a small risk of splenic abscess. Nonetheless, for those who cannot tolerate lifelong medication, PSE offers a durable middle ground.
Surgical Splenectomy
Removing the spleen outright is the most definitive way to stop platelet sequestration. In experienced centers, laparoscopic splenectomy carries a mortality rate below 2% and can raise platelet counts to >15010/L permanently. However, its a major operation with risks of infection, especially from encapsulated bacteria, so patients must receive appropriate vaccines beforehand.
Supporting Measures & Lifestyle Tweaks
While meds and procedures do the heavy lifting, everyday habits can tip the scales:
- Maintain a balanced diet rich in Bvitamins, folate, and ironall essential for healthy blood cell production. For people managing liver disease, attention to nutrition and related supplements (for example, exploring safe ulcerative colitis supplements in consultation with your clinician) can be part of a broader planthough always check compatibility with liver function.
- Avoid alcohol and hepatotoxic drugs; even occasional binge drinking can worsen portal hypertension.
- Some people report modest platelet boosts from beetroot juice or papaya leaf extract, but the evidence is limited; consider them complementary, not primary, therapies.
Want a quick action plan? Heres a short checklist you can print out and bring to your next appointment:
- Review current medicationsany drugs that thin blood (e.g., NSAIDs) should be discussed.
- Confirm recent labs: platelet count, liver enzymes, INR.
- Ask your hepatologist about eligibility for TPORA therapy.
- Discuss procedural timingsome treatments (like PSE) require a leadin period before the planned procedure.
- Update vaccinations if splenectomy is on the table.
Choosing the Right Approach
Every patients situation is unique, so the decision tree looks a bit like a ChooseYourOwnAdventure story. Lets break it down into four simple steps.
Assess Severity & Underlying Cause
Use the table above to locate your platelet range. If youre above 10010/L and not heading into a risky procedure, observation and lifestyle tweaks may be all you need. Below 5010/L? Its time to consider active treatment.
Factor in Comorbidities
Do you have liverrelated cancer, kidney disease, or a history of clotting disorders? Low platelets in the context of liver cancer (often termed low platelets liver cancer) may require a different balance of risk, especially if youre considering tumortargeted therapies that also affect blood clotting.
Weigh Benefits vs. Risks
Transfusions give an instant bump but are shortlived. TPORAs offer a steady climb but need monitoring for thrombosis. PSE sits in the middlemoderate durability with a mild recovery period. Splenectomy provides a permanent fix but carries surgical risks and lifelong infection vigilance.
Shared DecisionMaking Checklist
- What is my exact platelet count and trend?
- Do I need an upcoming procedure that mandates a higher count?
- Am I comfortable with daily oral medication, occasional injections, or a onetime procedure?
- What are my personal risk tolerances (e.g., avoiding surgery vs. avoiding longterm meds)?
- Do I have support for postprocedure care (e.g., for splenectomy vaccination schedule)?
Answering these questions with your doctor turns a vague treatment plan into a tailormade roadmap.
RealWorld Example
Consider Maria, a 58yearold with ChildPugh B cirrhosis and a platelet count of 4810/L. She needed a liver biopsy to evaluate for earlystage hepatocellular carcinoma. After reviewing options, her hepatologist prescribed lusutrombopag for 7 days before the biopsy. Her count rose to 7810/L, the procedure went smoothly, and she avoided a transfusion. A month later, her platelets stayed above 7010/L, allowing her to continue regular monitoring without further intervention.
Marias story highlights how a short course of a TPORA can bridge the gap between too low and just right, without the invasiveness of surgery.
Helpful Resources
When youre navigating cirrhosisrelated thrombocytopenia, credible sources make all the difference. The American Association for the Study of Liver Diseases (AASLD) publishes uptodate guidelines on managing portal hypertension and related blood disorders. offers detailed dosing tables for TPORAs, criteria for splenectomy, and monitoring recommendations. Keeping a bookmarked list of trusted sites can save you hours of Googling and help you ask the right questions at your next visit.
Conclusion
Living with cirrhosis and a low platelet count can feel like youre walking a tightrope, but you dont have to do it alone. Whether you opt for a quick transfusion, a course of thrombopoietin receptor agonists, a minimally invasive splenic embolization, or even a splenectomy, each pathway balances benefits and risks. The key is an honest conversation with your liver team, a clear understanding of where your counts sit, and a personalized plan that respects both your medical needs and your lifestyle preferences.
Take the checklist, explore the resources, and remember: you have options, you have support, and you have the power to make an informed choice. If youve tried any of these treatments or have questions about the next step, feel free to share your experience or reach out to a trusted liver specialistyoure not alone on this journey.
FAQs
What causes thrombocytopenia in cirrhosis?
Thrombocytopenia in cirrhosis is mainly caused by portal hypertension leading to spleen enlargement and platelet trapping, plus reduced thrombopoietin production by the damaged liver that lowers platelet creation in the bone marrow.
When is treatment for cirrhosis-related thrombocytopenia necessary?
Treatment is typically considered when platelet counts fall below 50×10⁹/L due to increased bleeding risk, especially before invasive procedures or surgeries.
What common treatments raise platelet counts in cirrhosis patients?
Treatment options include platelet transfusions for immediate but temporary improvement, thrombopoietin receptor agonists (like avatrombopag and lusutrombopag) for gradual sustained increase, partial splenic embolization, and surgical splenectomy for longer-lasting effects.
What are the risks associated with thrombopoietin receptor agonists?
While TPORAs effectively increase platelet production, potential risks include thrombosis, especially in patients with clotting history, and elevated liver enzymes requiring careful monitoring.
How should lifestyle changes support thrombocytopenia treatment in cirrhosis?
Maintaining a balanced diet rich in B vitamins, folate, and iron, avoiding alcohol and hepatotoxic drugs, and managing medications that affect blood clotting can support platelet health and overall liver function.