Lets cut to the chase:CNS relapse means that a cancermost often a type of leukemia or lymphomahas made its way back into the central nervous system (the brain, spinal cord, or the lining around them) after a period of remission. Its a heavy phrase, but understanding it early can be a gamechanger for patients, families, and anyone navigating this road.
If you or a loved one are facing a possible CNS relapse, youre probably feeling a mix of fear, confusion, and a desperate need for clear answers. Im here to walk you through what it means, whos most at risk, how doctors diagnose it, and what treatment options are on the table. Think of this as a friendly chat over coffeeno jargon, just straightforward info and a sprinkle of empathy.
What Is CNS Relapse
Definition & Clinical Criteria
A CNS relapse occurs when malignant cells appear again in the central nervous system after they have been cleared from the blood and bone marrow. Doctors look for two things:
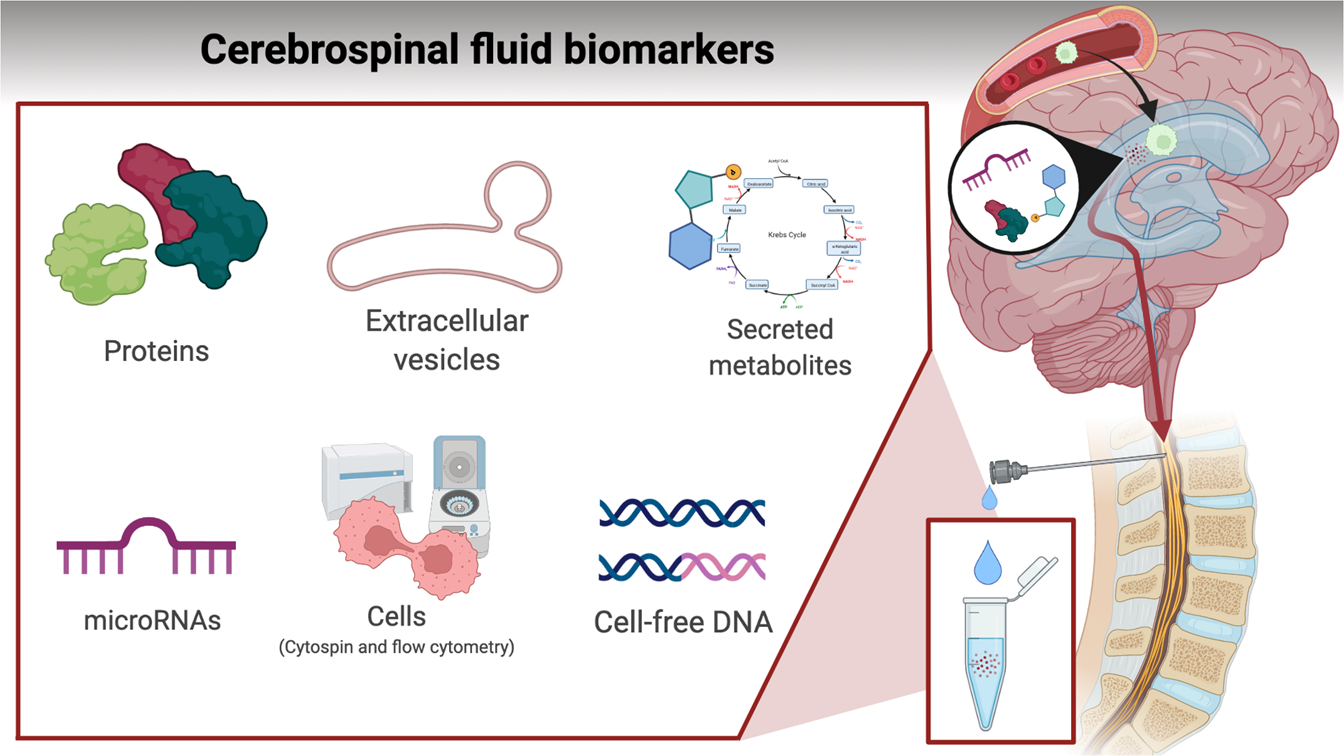
- Evidence of cancer cells in the cerebrospinal fluid (CSF) obtained via a lumbar puncture.
- Radiological signs on MRI or CT scanslike abnormal enhancement of the meninges or a new brain lesion.
Importantly, the relapse must involve the CNS itself; a tumor thats stuck to the spine's outer bone without penetrating the fluid spaces doesnt count as a true CNS relapse.
How Doctors Diagnose It
Diagnosis is a team effort. First, the oncologist will order a lumbar puncture to collect CSF. Lab technicians then run flow cytometry, PCR, or cytology to spot those sneaky leukemia or lymphoma cells. If the CSF is clear but symptoms persist, an MRI can reveal infiltrative disease thats lurking in the brain or meninges. Together, these tests confirm the diagnosis and help map the extent of the relapse.
RealWorld Example
Imagine a 32yearold patient named Maya, who had acute lymphoblastic leukemia (ALL) and underwent a successful stemcell transplant. Nine months later, she started experiencing occasional headaches and blurry vision. A lumbar puncture showed a few lymphoblasts, and an MRI highlighted subtle meningeal enhancement. Mayas team diagnosed a CNS relapse and promptly began intrathecal chemotherapy. Within weeks, her CSF cleared, and her symptoms receded. This vignette underscores how early detection can tip the balance toward a better outcome.
Who Is at Risk
Leukemia & Lymphoma Types
Not every blood cancer has the same chance of spreading to the CNS. Heres a quick snapshot:
| Disease | Typical CNS Relapse Rate | Key Risk Factors |
|---|---|---|
| ALL (pediatric) | 510% | Highrisk cytogenetics, CNSpositive at diagnosis |
| ALL (adult) | 812% | Age>35, high whitecell count |
| AML | 25% | Monocytic lineage, certain genetic abnormalities |
| Aggressive NHL | 48% | Testicular involvement, bulky disease, high LDH |
Specific Keywords in Context
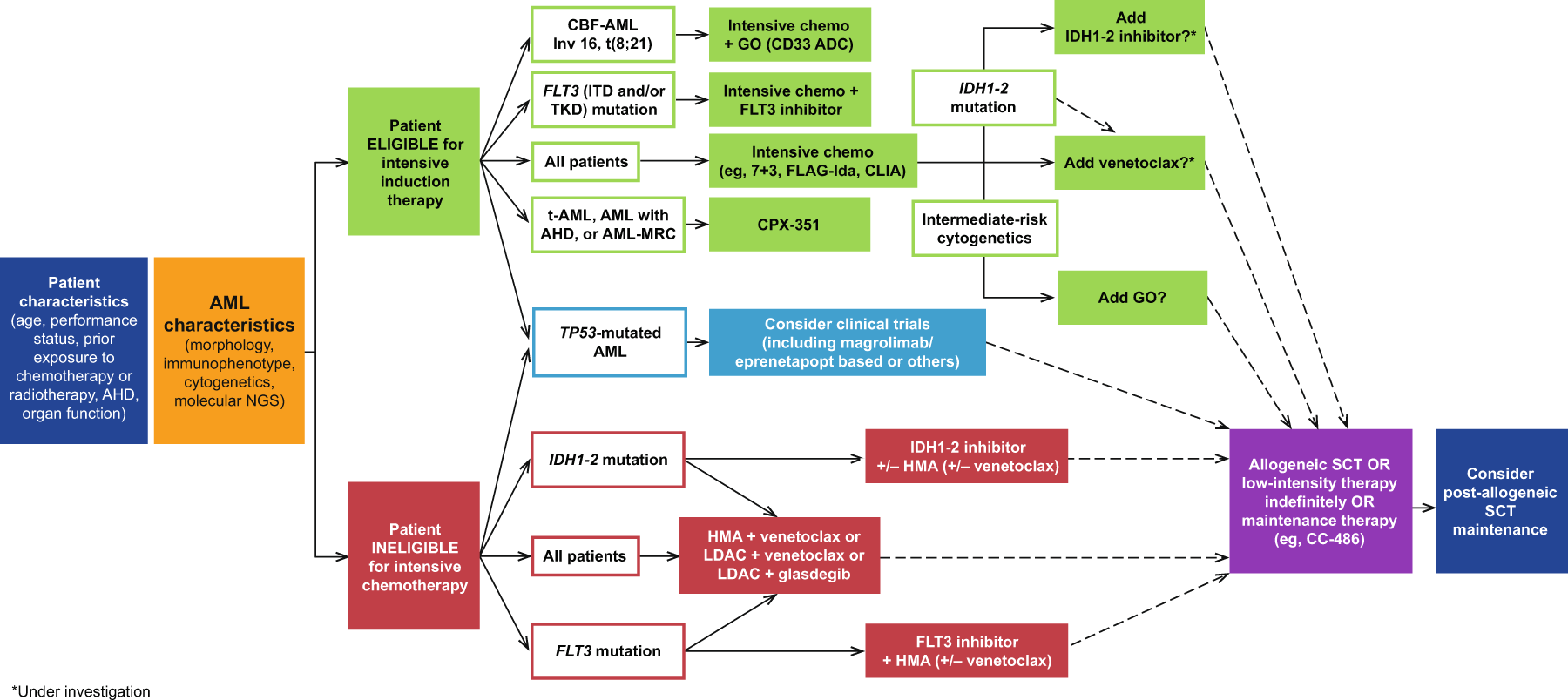
If youve searched for terms like aml cns relapse or cns involvement in leukemia, you were likely looking for how these diseases behave differently. AML, for example, tends to involve the CNS less frequently than ALL, but when it doesespecially with monocytic featuresthe prognosis can be more challenging. Thats why many oncologists incorporate cns prophylaxis in all treatment plans to head off the problem before it starts.
Treatment Paths
Standard FrontLine Therapies
When a CNS relapse is confirmed, the first line of attack usually combines systemic chemotherapy with intrathecal (directly into the CSF) drugs. Common intrathecal agents include methotrexate, cytarabine, and corticosteroids. The goal is twofold: flush out cancer cells from the CSF and penetrate any sanctuary sites in the brain.
RelapseSpecific Strategies
For patients who have already undergone intensive therapy, the approach shifts to salvage regimens. In the context of all relapse treatment, options might involve:
- Highdose systemic chemotherapy (e.g., FLAGIDA for AML).
- Targeted immunotherapies such as blinatumomab or inotuzumab, which have shown CNS activity.
- Radiation therapyeither cranial, craniospinal, or focalreserved for cases where chemo alone isnt enough.
Most centers also continue intrathecal prophylaxis during salvage to prevent a second CNS bounce. In discussions about overall outlook and survivorship it can also help to review information on related survivorship topics such as survival without prostate, which addresses qualityoflife considerations after major cancer treatments.
Emerging Options
Research is buzzing with new tools. , CART cell therapies that can cross the bloodbrain barrier are showing promise in refractory CNS disease. Likewise, CNSpenetrating small molecules like venetoclax, when combined with hypomethylating agents, are being explored in clinical trials for aml cns relapse.
When a Third Relapse Hits
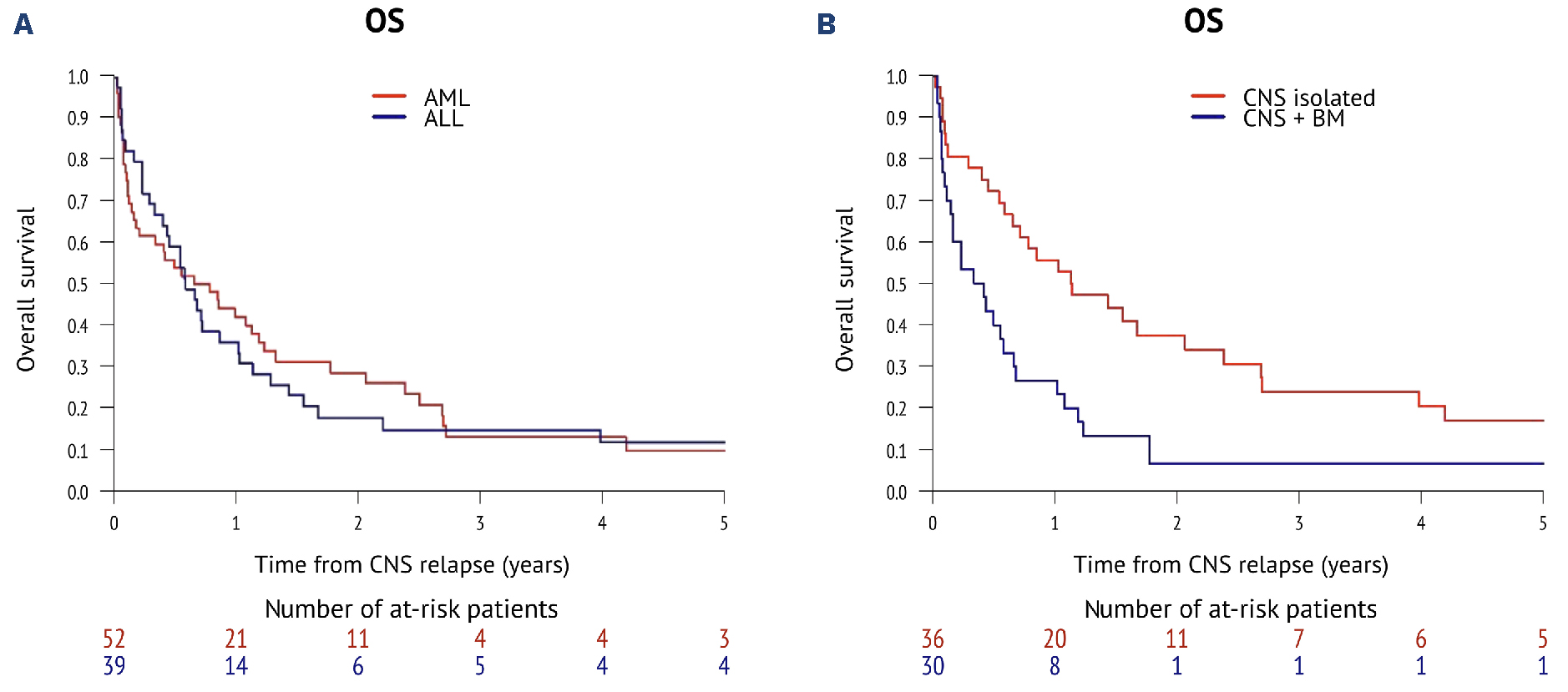
Prognosis and Statistics
Facing a third relapsewhether in ALL or AMLis daunting. Recent data from 2023 suggest a median overall survival of roughly 69months after a third CNS relapse, though outcomes improve markedly when a transplant is still an option and the patient retains good performance status.
DecisionMaking: Aggressive Cure vs. Palliation
At this stage, the conversation turns deeply personal. Doctors weigh the intensity of further chemo or a second transplant against qualityoflife considerations. Factors such as prior neurotoxicity, organ function, and the patients own goals become central. Its crucial to have open, honest talks with the care teamask about expected benefits, potential sideeffects, and what success looks like for you.
PatientFocused Checklist
- Watch for new headaches, vision changes, or neurologic deficits.
- Schedule regular CSF checksoften every 12months in highrisk settings.
- Keep a symptom diary to share with your oncologist.
- Discuss advance care planning early; its a sign of strength, not surrender.
Balancing Benefits & Risks
Why Early Detection Matters
Finding a CNS relapse before it causes major neurologic damage can preserve cognitive function, reduce the need for highdose radiation, and improve overall survival. Think of it like spotting a small leak earlyfixing it promptly saves you a flood later.
Potential SideEffects
Intrathecal chemotherapy isnt without downsides. Patients can experience chemical meningitis (headache, neck stiffness), transient neurocognitive changes, and, over the long term, endocrine disturbancesespecially in children whose brains are still developing.
Practical Tips for Families
Here are a few daytoday ideas to make the journey a bit smoother:
- Hydration is key: Staying wellhydrated helps CSF turnover, potentially reducing drug toxicity.
- Infection vigilance: Since lumbar punctures breach a sterile site, keep the insertion area clean and report fevers promptly.
- Mindbody support: Gentle yoga, guided meditation, or even simple breathing exercises can ease anxiety before a puncture.
Frequently Asked Questions (FeaturedSnippet Ready)
What does CNS relapse actually mean?
Its cancer that returns in the brain, spinal cord, or meninges after a period of remission.
How is it diagnosed?
Through detection of malignant cells in cerebrospinal fluid and/or abnormal findings on MRI/CT scans.
Can it be prevented?
Prophylactic intrathecal chemotherapy reduces risk but does not guarantee complete prevention.
Is CNS relapse the same in ALL and AML?
Both can spread to the CNS, but the patterns, incidence rates, and treatment nuances differ.
What are the newest treatments?
CART cell therapies that cross the bloodbrain barrier and CNSpenetrating targeted agents are at the forefront of research.
Sources & Further Reading
For those who want to dive deeper, consider checking reputable journals such as Haematologica and Leukemia. Patient advocacy groups like the Leukemia & Lymphoma Society also offer valuable resources and community support.
Conclusion
CNS relapse isnt just a medical termits a pivotal moment that can reshape a patients journey. By grasping the cns relapse meaning, recognizing early warning signs, and understanding the spectrum of treatment optionsfrom traditional intrathecal chemo to cuttingedge CART cellsyou empower yourself or a loved one to make informed, proactive choices. Remember, early detection can turn a daunting prognosis into a manageable challenge, and a balanced view of benefits versus risks keeps quality of life frontandcenter. If youre navigating this landscape, have questions, or simply need a listening ear, reach out to your oncology teamtheyre there to guide you every step of the way.
FAQs
What does CNS relapse mean?
CNS relapse refers to the return of cancer in the central nervous system—specifically the brain, spinal cord, or meninges—after a remission period.
How is CNS relapse diagnosed?
Doctors diagnose CNS relapse by detecting cancer cells in cerebrospinal fluid via a lumbar puncture and/or observing abnormal brain or meningeal changes on MRI or CT scans.
Who is at higher risk of CNS relapse?
Patients with certain blood cancers like acute lymphoblastic leukemia (ALL) and aggressive lymphomas have a higher risk, especially with specific genetic and clinical risk factors.
What treatments are commonly used for CNS relapse?
Treatments typically include intrathecal chemotherapy (drugs injected into cerebrospinal fluid), systemic chemotherapy, targeted immunotherapies, and sometimes radiation therapy.
Can CNS relapse be prevented?
Prophylactic intrathecal chemotherapy is used in many cases to reduce risk, but it does not guarantee complete prevention of CNS relapse.