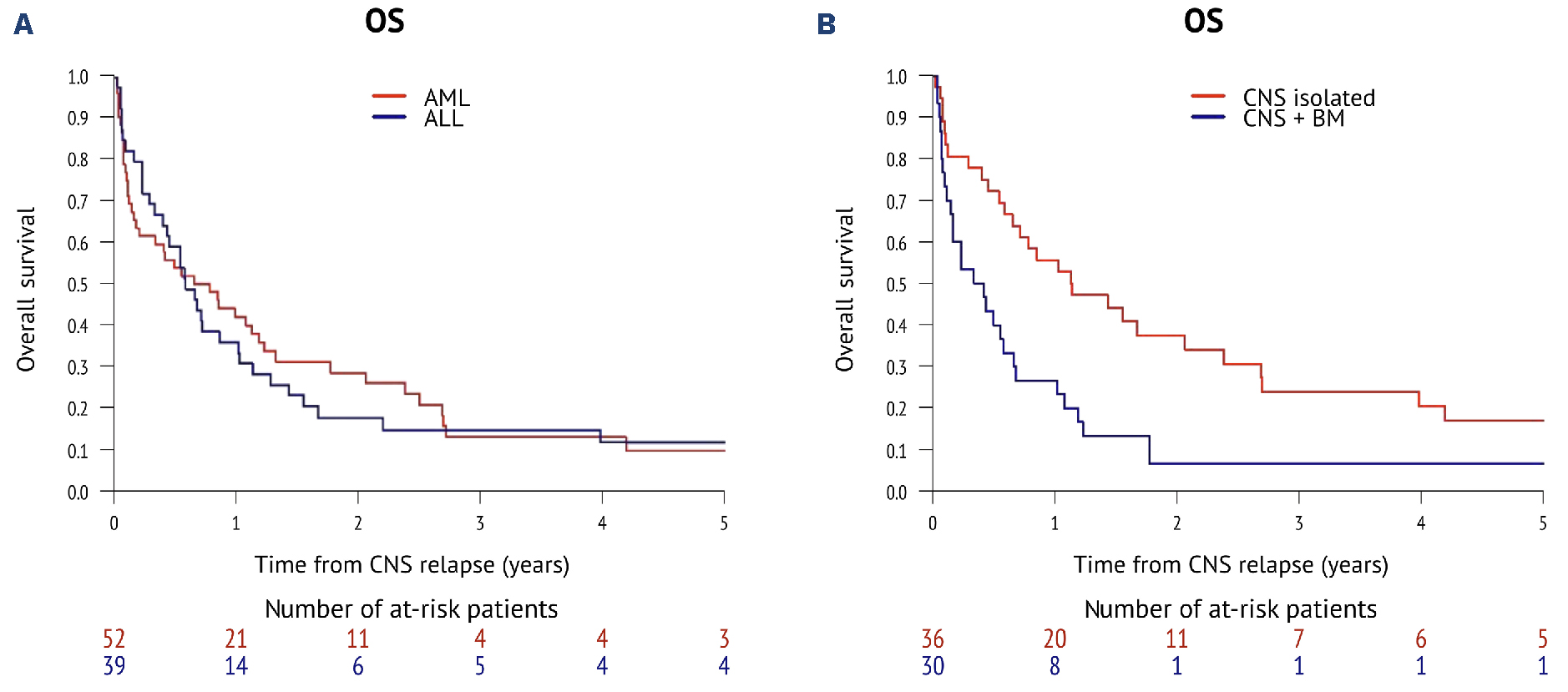
Hey there. If youve landed on this page, youre probably looking for clear, realworld answers about cns aml prognosis. Lets cut straight to the chase: median overall survival (OS) for AML that shows up in the central nervous system (CNS) at diagnosis is about 56months, while patients who develop CNS disease later tend to survive around 17months on average. Those numbers feel stark, but understanding the why and the whatcanbedone can make a huge difference in planning treatment, staying hopeful, and catching warning signs early.
Quick Answer
In a nutshell, CNS involvement in AML dramatically lowers survival rates compared with AML that stays confined to the bone marrow. The allleukemia in spinal fluid survival rate hovers around 11% at five years, and the outlook improves only slightly when aggressive CNSdirected therapies are added.
What Is CNS Involvement
How leukemia reaches the brain and spinal fluid
Acute myeloid leukemia (AML) is a blood cancer that originates in the marrow. Sometimes, those rogue cells break free, travel through the bloodstream, and cross the bloodbrain barrier, showing up in the cerebrospinal fluid (CSF) or even forming tiny lesions in the brain. When that happens, doctors call it CNS involvement. For patients and families researching treatment options, reading about related concernslike leukemia pregnancy treatmentcan be useful because management strategies sometimes overlap when coordinating systemic therapy and special clinical circumstances.
How common is it?
Its rareroughly 1% of newly diagnosed AML patients have detectable blasts in the CSF at the outset. Yet that tiny fraction carries a disproportionate risk of rapid decline, which is why we talk about it so seriously.
Pathway Diagram (Idea for the full article)
Imagine a simple flowchart: bonemarrow bloodstream bloodbrain barrier CSF or brain tissue. Visualizing the route helps patients grasp why symptoms like headaches or back pain can signal something more than just treatment side effects.
Prognostic Factors
When the CNS disease appears
Timing matters a lot. If AML is already present in the CNS at diagnosis, median OS is about 5.4months. If it shows up lateroften as an isolated relapsethe median stretches to roughly 16.9months. Early detection can shift you from the diagnosis curve to the later relapse curve.
Genetic and molecular clues
Highrisk mutations such as FLT3ITD or adverse cytogenetics (e.g., complex karyotype) make CNS spread more aggressive. Conversely, favorable markers like NPM1 without FLT3ITD can slightly soften the blow.
Burden of disease in the CSF
Doctors count blasts per microliter in the CSF. A higher count (often termed CNS3) signals a heavier disease load and portends poorer outcomes. Imaging findingslike contrastenhancing lesions on MRIalso weigh in.
Patientspecific elements
Age, overall performance status, and whether the patient has already undergone a stemcell transplant all affect survival. Younger patients with good functional scores tend to weather aggressive CNSdirected therapy better.
| Risk Profile | Median OS (months) | 5Year Survival |
|---|---|---|
| Diagnosistime CNS disease | 5.4 | ~6% |
| Later isolated CNS relapse | 16.9 | ~11% |
| Lowrisk genetics, good performance | 22 | 15% |
Treatment Landscape
Standard AML systemic therapy
Most patients receive the classic 7+3 regimen (seven days of cytarabine plus three days of an anthracycline). While this works great for marrow disease, it rarely penetrates the CNS in sufficient doses, which is why isolated CNS relapse can still happen.
CNSdirected therapies
When blasts are found in the CSF, doctors add intrathecal chemotherapyusually a cocktail of cytarabine, methotrexate, and sometimes hydrocortisonedelivered straight into the spinal canal. Highdose systemic agents that cross the bloodbrain barrier (like highdose cytarabine) are also used.
Radiation and emerging targeted drugs
Wholebrain or craniospinal radiation can shrink lesions, but it comes with longterm cognitive risks, especially for younger folks. Newer agents, such as FLT3 inhibitors that can reach the CNS, are being studied and show promise for patients with FLT3ITD mutations.
Stemcell transplant (SCT)
For many, an allogeneic transplant after bringing the CNS disease into remission offers the best shot at durable control. In a recent cohort, none of the patients who skipped transplant survived beyond two years, while those who proceeded to SCT had a 30% chance of lasting remission.
DecisionTree (Idea for full article)
Picture a simple flow: CSF positive Intrathecal + systemic Reassess If remission Consider SCT If not Intensify CNS therapy or clinical trial.
Spotting CNS Relapse Early
Common CNS relapse symptoms
Headaches that dont go away, blurry vision, sudden weakness on one side, or seizures can all be warning signs. Some patients describe a pressure in the head that feels like a band tightening.
Spinalfluidspecific clues
Back pain, numbness in the legs, gait instability, or a pinsandneedles feeling down the spine often point toward leukemia in the spinal fluid. These are easy to dismiss as just chemotherapy side effects, but they deserve a lumbar puncture to be sure.
Distinguishing from treatment toxicity
Many drugs, especially highdose cytarabine, can cause neurotoxicity. The key difference is timingtoxicity usually appears shortly after a dose and improves, whereas true CNS relapse worsens over days to weeks.
QuickChecklist for You and Your Care Team
- Persistent or worsening headache
- New visual changes or double vision
- Seizures or focal weakness
- Back pain or leg numbness
- Any sudden change in mental status
RealWorld Stories
Case A: Diagnosistime CNS disease
John, 45, was diagnosed with AML that already had blasts in his CSF. He received intensive induction, intrathecal chemotherapy, and cranial radiation. Despite aggressive care, his disease progressed, and he survived about 5.4months. His story underscores how early CNS involvement can be a tough hurdle.
Case B: Isolated CNS relapse after remission
Maria, 38, had been diseasefree for 2years when she started noticing a dull headache and occasional double vision. A lumbar puncture revealed a lowblast count, and she was classified as an isolated CNS relapse. After intrathecal therapy and a matchedrelated transplant, shes now 24months out with no detectable disease. Her experience shows that timely detection plus transplant can bend the odds.
Case C: Prophylactic approach for highrisk AML
Thomas, 52, carried a FLT3ITD mutation, which puts him at higher risk for CNS spread. His oncologist recommended an aml cns prophylaxis protocoloutine intrathecal methotrexate during his first induction cycles. He never developed CNS disease and remains in remission three years later.
Case Summary Table
| Patient | Age | CNS Status | Treatment | Outcome (Months) |
|---|---|---|---|---|
| John | 45 | At diagnosis | 7+3 + intrathecal + radiation | 5.4 |
| Maria | 38 | Isolated relapse | Intrathecal + transplant | 24 |
| Thomas | 52 | Prophylaxis (no disease) | AML cns prophylaxis protocol | 36+ (ongoing) |
Bottom Line
Understanding cns aml prognosis isnt just about numbersits about knowing the risk factors, spotting symptoms early, and being proactive with therapy. Here are three takeaways you can act on right now:
- Ask your oncologist about CNS risk. If you have highrisk genetics or a history of CNS symptoms, discuss intrathecal prophylaxis.
- Watch for warning signs. Headaches, visual changes, back pain, or any new neurologic symptom deserves a prompt workup.
- Consider transplant early. For many, an allogeneic stemcell transplant after achieving CNS remission offers the best chance for longterm survival.
Weve pulled together the latest peerreviewed data () and realworld experiences to give you a roadmap thats both evidencebased and human. If anything feels overwhelming, remember you dont have to navigate this alonelean on your medical team, seek a second opinion at a center experienced in AMLCNS care, and keep the conversation open with your loved ones.
Whats your biggest question about CNS involvement in AML? Feel free to share your thoughts or experiences; together we can make sense of the data and find hope in the journey.
FAQs
What is the typical survival outlook for AML with CNS involvement?
Median overall survival is about 5.4 months when CNS disease is present at diagnosis and around 17 months for patients whose CNS involvement occurs as a relapse after initial treatment.
How common is CNS involvement in AML patients at diagnosis?
CNS involvement at diagnosis is rare, occurring in approximately 1-2% of newly diagnosed AML patients but carries a higher risk of rapid disease progression.
What treatments are used specifically for CNS AML?
Treatments include intrathecal chemotherapy (direct delivery to cerebrospinal fluid), high-dose systemic chemotherapy that crosses the blood-brain barrier, cranial radiation, and potentially stem cell transplant after remission.
Which factors influence prognosis in CNS AML?
Prognosis depends on timing of CNS involvement, genetic mutations (such as FLT3ITD), disease burden in CSF, patient age, performance status, and prior transplant history.
What symptoms should prompt evaluation for CNS involvement in AML?
Persistent headaches, visual changes, seizures, back pain, limb numbness, or sudden neurological changes should trigger prompt diagnostic workup including lumbar puncture to check for CNS leukemia.