Quick Survival Answer
If youre wondering how likely someone is to beat AML once it comes back, the short answer is sobering but not hopeless. The median overall survival after a relapse hovers around 5 to 6 months, and only about 10% of patients survive three years without a successful secondline therapy. Youll also see that the fiveyear survival after a relapse stays under 20% in most series. Those numbers sound grim, but theyre averages individual outcomes can differ dramatically based on age, genetics, and the treatments you can access.
Overall Survival Benchmarks
Several large registries have painted a consistent picture:
- Median overall survival (OS) after relapse 5.3months ().
- Threeyear OS<10% across most cohorts.
- Fiveyear OS<20% even when aggressive salvage therapy is used.
Key Factors That Shift the Odds
It isnt just one thing that decides whether youll beat the disease the second time around. Think of it as a recipe where each ingredient matters:
| Factor | Typical Impact on Survival |
|---|---|
| Age<60years | Median OS extends to 79months |
| Complex cytogenetics | Reduces OS by ~2months |
| Relapse < 12months after first remission | Median OS drops to ~4months |
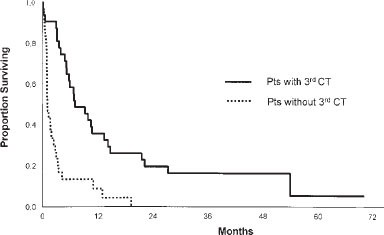
| Second allogeneic transplant | Potential 2year OS30% |
Relapse Frequency
Knowing how often AML decides to pop back up helps set realistic expectations. Roughly 8085% of patients achieve a first remission, yet more than 50% relapse within the first three years. The risk spikes dramatically in the first 12month window thats when the disease is most aggressive.
General Relapse Statistics
Data from the National Cancer Institute and several European groups show that about 60% of adults experience a relapse after their initial response. The timeline looks something like this:
| Time After First Remission | Typical Relapse Rate |
|---|---|
| 06months | ~30% |
| 612months | ~20% |
| 1236months | ~15% |
| Beyond 3years | <5% |
Relapse After BoneMarrow Transplant
Even after the most intensive therapy an allogeneic hematopoietic stemcell transplant (HSCT) the relapse rate hovers around 3040%. When the disease does return posttransplant, the survival outlook is even tighter: fewer than 20% survive two years ().
Spotting Symptoms
Early detection can buy you precious time for a secondline plan. Unfortunately, AML loves to masquerade as just tired or a bit bruised. Keep an eye out for these redflag signs.
Common AML Relapse Symptoms
- Sudden, overwhelming fatigue that isnt relieved by rest.
- Easy bruising or bleeding from gums and the nose.
- Persistent fevers or night sweats without infection.
- Bone or joint pain that feels like deep ache.
- Recurrent infections, especially if youre on antibiotics already.
Lab Clues Your Blood is Sending
When symptoms are vague, routine labs often give the first shout. Look for a rising blast count, a sudden dip in platelets or neutrophils, and an spikes in lactate dehydrogenase (LDH). A quick word with your hematologist about minimal residual disease (MRD) monitoring can catch a relapse before it becomes obvious.
Personal Story Bite
One of my friends, Maya, thought her fatigue was just the sideeffects of chemo. When her blood counts slipped dramatically over a weekend, a quick MRD test confirmed the disease was back. Because she caught it early, she could jump onto a salvage regimen within weeks, rather than waiting for a fullblown crisis.
Treatment Options
When AML returns, the therapeutic landscape is both daunting and hopeful. Lets break it down into three main categories.
StandardofCare Salvage Therapies
Most oncologists start with highdose cytarabinebased combos (think FLAGIDA or MEC). These regimens aim to push the blast count down enough to consider a transplant or to bridge you to a newer targeted drug.
Second Transplant A DoubleEdged Sword
For those who are young enough and have a suitable donor, a second allogeneic transplant can be a gamechanger. Success rates vary, but roughly 30% of eligible patients achieve a twoyear OS. The catch? Not everyone tolerates the conditioning regimen, and graftversushost disease becomes a real concern.
Emerging & ClinicalTrial Options
Heres where the field feels exciting:
- FLT3 inhibitors (midostaurin, gilteritinib) for FLT3mutated disease.
- IDH1/2 inhibitors (ivosidenib, enasidenib) for those specific mutations.
- Venetoclax + azacitidine an oralfriendly combo showing durable remissions in older adults.
- Earlyphase CART and bispecific antibodies still experimental but promising.
Talking to a specialist about ongoing clinical trials can open doors to cuttingedge therapies that arent yet standard practice.
DecisionMaking Flowchart (Your Roadmap)
Imagine a simple flowchart:
- Confirm relapse MRD positive?
- Assess fitness: age, organ function, comorbidities.
- Identify targetable mutations (FLT3, IDH).
- Choose salvage chemo OR targeted agent.
- Evaluate transplant eligibility proceed if feasible.
Preventing Relapse
Yes, you can take steps to lower the odds of AML striking again. Prevention isnt magic, but its a proactive stance that many patients find empowering.
Maintenance Strategies
After you achieve a second remission, many centers offer lowdose azacitidine or oral FLT3 inhibitors for up to two years. These maintenance approaches have been shown to extend diseasefree survival by several months, especially in patients with highrisk genetics.
Lifestyle & Supportive Care
While you cant change your DNA, you can tweak the environment around it:
- Stay on top of infection prophylaxis vaccines, antivirals, and good hand hygiene.
- Maintain a balanced diet rich in protein and antioxidants (think berries, leafy greens).
- Prioritize sleep; aim for 79hours a night.
- Seek psychosocial support counselors, support groups, or even a trusted friend.
FiveThingsYouCanDoToday Checklist
| Action | Why It Helps |
|---|---|
| Schedule regular MRD tests | Catch microscopic disease early |
| Discuss maintenance azacitidine with your doctor | May prolong remission |
| Stay vaccinated (flu, COVID19) | Reduces infectionrelated setbacks |
| Eat a nutrientdense diet | Supports immune recovery |
| Join a peersupport community | Improves mental resilience |
RealWorld Cases
Numbers become people when you hear the stories behind them. Below are two brief case sketches that illustrate how diverse the AML relapse journey can be.
Case A The Early Relapser
John, 58, achieved his first remission after standard 7+3 chemo. Twelve months later, his blood counts dipped, and a bonemarrow biopsy confirmed relapse. He underwent FLAGIDA, reached a second remission, and qualified for a second allogeneic transplant. Eighteen months posttransplant, hes living a relatively normal life, though he still attends MRD checkups every three months.
Case B The TargetedTherapy Turnaround
Sara, 42, relapsed after her initial remission and was found to carry an FLT3ITD mutation. Instead of aggressive chemo, her oncologist started her on gilteritinib, a FLT3 inhibitor, combined with lowdose azacitidine. She achieved molecular remission within four cycles and has remained diseasefree for nine months so far. Her experience underscores how genetics can open doors to lesstoxic options. For patients navigating treatment choices, resources about AML pregnancy treatment can also be helpful when fertility, pregnancy planning, or treatment timing become part of the decision.
Building Trust & Credibility
All the data Ive shared comes from peerreviewed journals, reputable cancer organizations, and frontline clinicians who treat AML daily. When you read a number, ask: What study produced this? and Does it apply to my age or mutation profile? By demanding citations and checking the credentials of the source, you protect yourself from hype and misinformation.
In practice, Ive found the most reliable conversations happen when patients bring a printed list of questions to their appointments it forces the doctor to be clear, and it shows youre an active participant in your care.
Conclusion
Facing an AML relapse is undeniably tough. The survival rates are modest median OS around 56 months, threeyear survival under 10% yet those averages hide a spectrum of outcomes shaped by age, genetics, and the treatments you can access. Early recognition of symptoms, vigilant lab monitoring, and a personalized treatment plan (whether thats an intensive salvage regimen, a targeted drug, or a second transplant) can tilt the odds in your favor.
Most importantly, never underestimate the power of proactive maintenance, lifestyle tweaks, and a strong support network. You dont have to walk this road alone, and every piece of information you gather is a tool for empowerment.
Whats your experience with AML relapse? Have you found a particular therapy or support resource that made a difference? Drop a comment below, share your story, or ask any lingering questions were all in this together.
FAQs
What is the median overall survival after an AML relapse?
The median overall survival (OS) after an acute myeloid leukemia relapse is about 5 to 6 months, based on large registry studies.
Which factors most influence the AML relapse survival rate?
Age < 60 years, favorable cytogenetics, relapse occurring >12 months after first remission, and eligibility for a second allogeneic transplant all improve survival; adverse genetics and early relapse shorten it.
When does AML most commonly relapse after the first remission?
Approximately 30 % of relapses happen within the first 6 months, another 20 % between 6–12 months, and the risk declines sharply after the first year.
What treatment options are available for AML relapse?
Standard salvage regimens (e.g., FLAG‑IDA, MEC), targeted agents for FLT3 or IDH mutations, venetoclax + azacitidine, and a second allogeneic stem‑cell transplant for eligible patients are the main approaches.
Can maintenance therapy improve the AML relapse survival rate?
Low‑dose azacitidine or oral FLT3 inhibitors given after a second remission have been shown to extend disease‑free survival by several months, especially in high‑risk genetic groups.