Quick Answer Overview
In a nutshell, the TNM system breaks stomach (gastric) cancer into three simple parts T for the size and depth of the primary tumor, N for nearby lymphnode involvement, and M for distant spread. Combine those three letters and numbers and you get a stage from 0 toIV. The stage tells doctors how far the disease has traveled and, more importantly, which treatments stand the best chance of helping you. For patients also navigating other cancer diagnoses, resources about prostate cancer outlook may offer useful context on prognosis communication and supportive care planning.
Tumor (T) Details
What does T actually measure?
T looks at how deep the cancer has invaded the stomach wall. Think of the stomach as a layered cake: the inner lining (mucosa), a thin muscular layer (submucosa), the muscle itself (muscularis), and the outer covering (serosa). A T1 tumor is still in the top one or two layers, while a T4 tumor has breached the serosa and may be touching nearby organs.
Realworld example of a T2 tumor
Imagine a friend, Maria, who just got a pathology report after a biopsy. The report says T2 tumor invades the muscularis propria. In plain English, the cancer has reached the muscle layer but hasnt yet poked through the outer wall. That information helps her surgeon decide whether a minimally invasive removal might be enough.
Table: TCategory vs. Stomach Wall Layer
| TCategory | Depth of Invasion |
|---|---|
| T0 | No evidence of primary tumor |
| T1 | Mucosa or submucosa |
| T2 | Muscularis propria |
| T3 | Serosa (outermost layer) |
| T4 | Beyond serosa adjacent organs |
Node (N) Details
How do we count the nodes?
N is all about the lymphnode highway. N0 means no cancer found in any examined nodes. N1 indicates 12 nodes, N2 is 36 nodes, and N3 means 7 or more. The higher the number, the greater the chance the disease has taken a shortcut to distant sites.
A surgeons perspective on an N1 finding
When Dr. Patel, a surgical oncologist, says your pathology shows N1 disease, shes telling you that a few nearby nodes contained cancer cells. That might change the plan from surgery alone to adding chemotherapy before or after the operation.
Comparison: NStage vs. Risk of Distant Spread
| NStage | Typical Risk of Metastasis |
|---|---|
| N0 | Low (1015%) |
| N1 | Moderate (3040%) |
| N2 | High (5060%) |
| N3 | Very high (70%) |
Metastasis (M) Details
What does M1 mean for a patient?
M0 means no distant spread the cancer is still hanging out in the stomach and nearby nodes. M1 says weve found it elsewhere, most often in the liver, peritoneum, or lungs. Thats the hallmark of stageIV, the last stages of stomach cancer.
How radiology catches M1 disease
Modern imaging, especially PET/CT and contrastenhanced MRI, can spot tiny lesions that a CT scan might miss. According to a recent review in , PET/CT improves detection of distant metastases by roughly 20% compared with CT alone.
Quick checklist for patients
When you meet your oncologist, ask:
- Did we do a PET/CT or MRI to look for Mstatus?
- What organs are most likely to host metastases in my case?
- If M1 is present, what systemic options are on the table?
Overall Cancer Stages
How do T, N, and M combine?
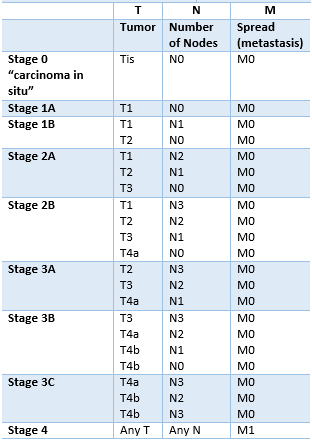
The American Joint Committee on Cancer (AJCC) stitches the three letters into the familiar stage numbers. Heres a quick mental map:
- Stage0: Tis, N0, M0 carcinoma in situ, no invasion.
- StageI: Small T (T1T2) with N0, M0 early disease.
- StageII: Larger T (T3) or limited N (N1) but still M0.
- StageIII: Any T with N2N3, still M0 locally advanced.
- StageIV: Any T, any N, M1 distant spread.
This layout is drawn straight from the guide, the gold standard for oncologists worldwide.
Visual flowchart (conceptual)
Picture a decision tree: start with T, branch to N, then check M. Follow the arrows, and you land on a stage number that determines the next therapeutic step.
8th Edition Updates
What changed in the newest edition?
The 8th edition of the AJCC staging manual refined a few key points:
- It split the N category into N1a (12 nodes) and N1b (36 nodes) for better prognostic granularity.
- It introduced a substaging for T4 tumors based on whether the invasion is into the pancreas versus the colon.
- It added the concept of grade (how abnormal the cells look) as a complementary factor, though not part of the TNM code itself.
These tweaks help doctors predict outcomes more accurately especially when combined with modern pathology outlines (tnm staging stomach cancer pathology outlines) that include molecular markers.
Treatment By Stage
Early stages (0I): Surgery or endoscopy?
If youre in stage0 or I, the cancer is usually confined to the inner layers. Many patients qualify for endoscopic submucosal dissection (ESD), a minimally invasive cutandremove that spares the stomach. If the tumor is a bit larger, a simple gastrectomy (partial stomach removal) often cures the disease.
Intermediate stages (IIIII): Multimodal approach
When the cancer has reached the muscle or a few nodes, surgery alone rarely suffices. The current standard includes perioperative chemotherapy (before and after surgery) a regimen like FLOT (5fluorouracil, leucovorin, oxaliplatin, and docetaxel) has shown a 30% boost in survival compared with surgery alone ().
Advanced stage (IV): Systemic therapy and palliation
When M1 is present, the focus shifts to controlling disease spread and quality of life. Options include:
- Systemic chemotherapy (often with a fluoropyrimidinebased backbone).
- Targeted therapies for HER2positive tumors.
- Clinical trials that explore immunotherapy or novel agents.
- Palliative surgery or radiation to relieve obstruction or bleeding.
Even in the last stages of stomach cancer, many patients experience meaningful symptom relief and sometimes a surprise plateau in tumor growth.
Checklist for patients navigating treatment
Ask your care team:
- What is the exact TNM stage of my tumor?
- Which clinical trials are open for my stage?
- How will we monitor response to therapy?
- What supportive services (nutrition, counseling) are available?
Survival By Stage
What does life expectancy look like?
Survival rates vary dramatically by stage. According to recent data from the :
- Stage0I: 5year survival exceeds 8090%.
- StageII: About 6070% survive five years.
- StageIII: Roughly 3040% make it to five years.
- StageIV: Median overall survival is around 1215months, but some patients live longer with aggressive therapy.
These numbers are averages; many personal factorsage, overall health, tumor biologycan push them up or down. Thats why detailed staging (the tnm staging gastric cancer (8th edition)) matters so much.
Factors that improve outlook
Early detection, participation in clinical trials, and a multidisciplinary team approach all correlate with better outcomes. Even lifestyle measuresbalanced nutrition, regular exercise, and smoking cessationcan bolster your bodys ability to tolerate treatment. For patients interested in nutritional strategies during cancer care, see guidance on a cancer diet plan to support strength and treatment tolerance.
Resources & Next Steps
Where to find reliable information
When youre navigating a diagnosis, trusted sources are like a lighthouse in fog. Good places to start include:
- The Canadian Cancer Societys stomach cancer staging page.
- The National Cancer Institutes (NCI) Gastric Cancer overview.
- Professional societies such as the Society of Surgical Oncology for patientfocused guides.
How to talk to your doctor about TNM results
Bring a notebook, ask clear questions, and dont be shy about requesting clarification. For example: Can you walk me through each part of my TNM stage and what it means for my treatment options?
Support groups and community help
Connecting with people whove walked a similar path can be incredibly reassuring. Look for local meetups, online forums moderated by cancer centers, or national organizations that offer counseling and peersupport programs.
Takeaway checklist
Before you close this page, check off these actions:
- Confirm your exact TNM stage with your oncology team.
- Download a printable staging cheatsheet (many hospitals provide one).
- Ask about clinical trial eligibility.
- Identify at least one support resource youll reach out to.
Remember, the letters T, N, and M are just a language doctors use to describe where the tumor is. Understanding that language gives you powerpower to ask the right questions, to make informed decisions, and to stay hopeful even when the road looks tough.
Whats your experience with stomachcancer staging? Have you found a particular resource or question that helped you feel more in control? Share your thoughts in the comments below, and lets keep this conversation going. If you have any lingering questions, dont hesitate to askyour curiosity is an essential part of navigating this journey.
FAQs
What does each part of the TNM staging system represent for stomach cancer?
The “T” indicates how deep the tumor has invaded the stomach wall, “N” shows how many nearby lymph nodes contain cancer cells, and “M” reveals whether the cancer has spread to distant organs.
How is the T category determined in gastric cancer?
Pathologists examine the depth of invasion: T1 is limited to the mucosa or submucosa, T2 reaches the muscularis propria, T3 extends to the serosa, and T4 breaks through the serosa into adjacent structures.
What is the significance of N1 vs N2 lymph‑node involvement?
N1 means 1‑2 nodes are positive, N2 means 3‑6 nodes. Higher N numbers increase the risk of distant metastasis and usually prompt the addition of chemotherapy to surgery.
How do doctors detect M1 disease in stomach cancer patients?
Advanced imaging such as PET/CT or contrast‑enhanced MRI is used to look for distant lesions in the liver, peritoneum, lungs, or other organs. Positive findings are classified as M1.
What treatment options are recommended for stage III stomach cancer?
Stage III is treated with multimodal therapy: peri‑operative chemotherapy (e.g., FLOT regimen) combined with surgery, and sometimes postoperative radiation, to improve survival.