If youre past fifty and still battling pelvic pain, uncomfortable bathroom trips, or strange hotflashlike sensations, you might wonder whether endometriosis could still be part of the picture. The short answer is: yes, it can. Even after the natural decline of estrogen, endometriosis can linger, morph, or even flare up, showing up as a mix of familiar menopausal complaints and some very specific redflag signs.
Below youll find a friendly, indepth walkthrough of the most common menopause endometriosis symptoms, why they appear, how doctors figure them out, and what treatment paths are safest for a postmenopausal body. Grab a cup of tea, settle in, and lets demystify this together.
Quick Answer Overview
In a nutshell, the key signs to keep an eye on are:
- Pain in the lower abdomen or pelvis that isnt eased by typical menopause remedies.
- Unexplained changes in bowel habits frequent diarrhea, constipation, or sudden bloating.
- Painful or urgent urination without a clear infection.
- Occasional postmenopausal spotting or bleeding.
- Hot flashes that feel different and dont respond well to hormonereplacement therapy (HRT).
Seeing any of these? Its worth chatting with a specialist who can rule out (or confirm) endometriosis.
Why It Persists
What Happens to Endometriosis After Menopause?
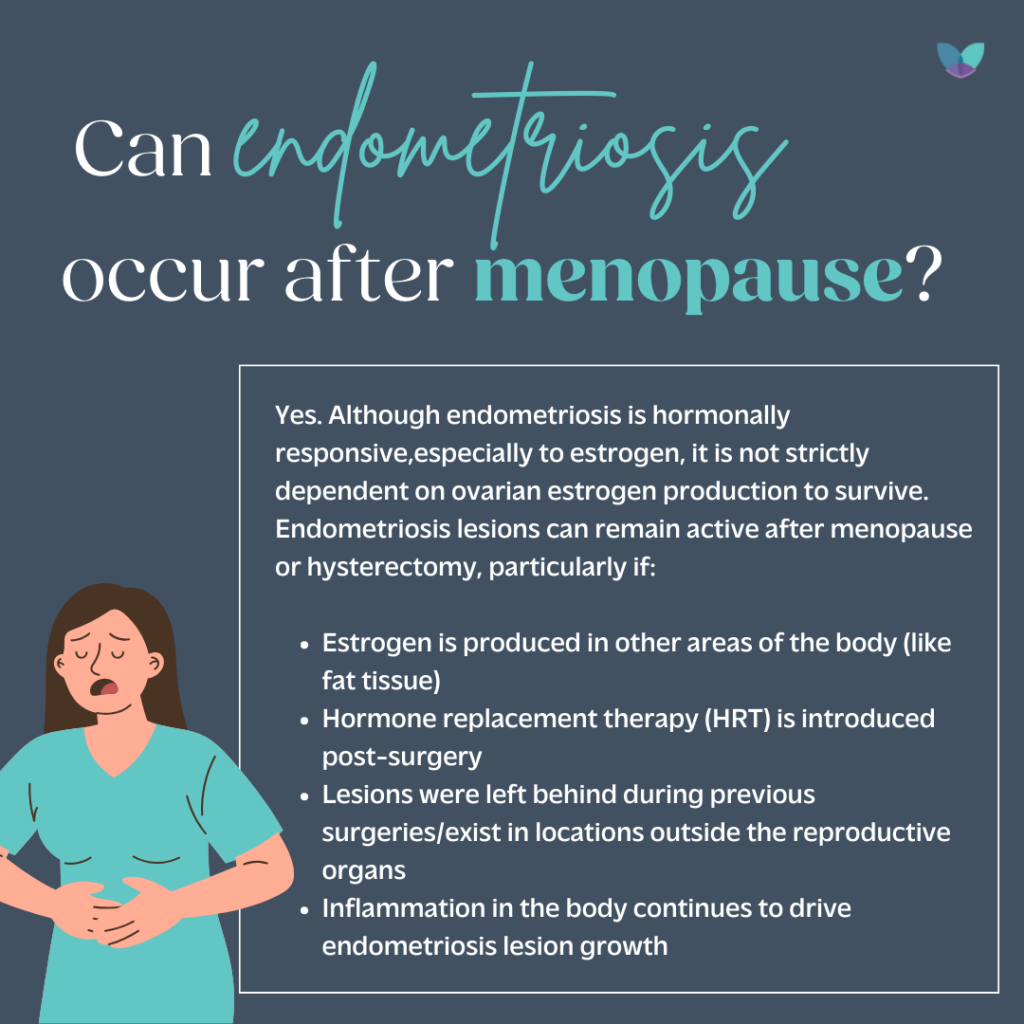
Many people assume that once estrogen levels drop, the condition simply disappears. In reality, endometrial tissue can become quiescent, but it doesnt always vanish. Residual lesions may stay dormant for years, then reactivateespecially if youre on HRT or have other hormonal fluctuations. A recent review in notes that up to 15% of women with a history of endometriosis report symptoms after menopause.
Does Menopause End Endometriosis?
This is a common myth. While the intensity often eases, the disease can linger. Think of it like a garden: even after the main watering stops, some hardy weeds can survive and sprout again when the conditions are right.
How AgeRelated Factors Influence Symptom Expression
Our bodies change with agemuscle tone, pelvic support, and even the way nerves transmit pain. All of these can amplify or mask the signals coming from lingering endometrial tissue. For example, scar tissue from previous surgeries may tug on surrounding organs, creating discomfort that feels new even though the source is old.
Core Symptoms Overview
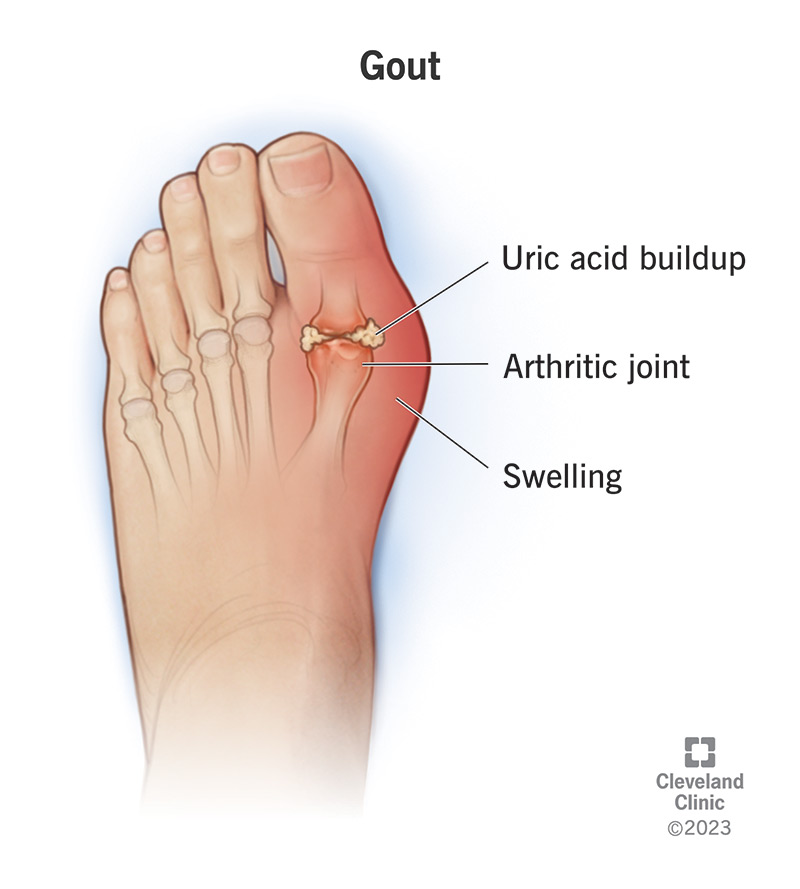
Pelvic & Abdominal Pain Patterns
Postmenopausal pain often feels deeper and more constant than the cramping you might have experienced in your 30s. It may radiate to the lower back or thighs, and it usually worsens during movement, intercourse, or after a heavy meal.
Bowel Endometriosis After Menopause
The intestinal tract is a frequent playground for hidden lesions. If you notice sudden bouts of diarrhea, constipation, or a persistent sense of fullness, it could be bowel endometriosis. Below is a quick sidebyside comparison with irritable bowel syndrome (IBS), a condition that often masquerades as the same thing.
| Feature | Endometriosis | IBS |
|---|---|---|
| Pain timing | Worsens with menstrualtype hormone shifts, often during or after sex | Often related to meals, stress, or specific foods |
| Bleeding | Occasional rectal bleeding if deep lesions erode tissue | Rare |
| Response to hormonal meds | Improvement with progestins or GnRH analogues | No effect |
| Imaging clues | MRI shows thickened bowel wall or nodules | Usually normal |
Bladder Endometriosis After Menopause
Imagine thinking you have a recurrent urinary tract infection, only to discover a tiny spot of endometrial tissue irritating the bladder wall. Painful urination, urgency, and even occasional blood in the urine are classic signals. One patient I heard about described it like my bladder was constantly on edgelike a tiny alarm that never turned off.
MenopausalLike Signs That Might Be Endometriosis
Hot flashes are a hallmark of menopause, but when they come paired with pelvic pain or bowel changes, they could be a red flag. Endometriosis can produce estrogen locally, leading to false hot flashes that dont calm down with standard HRT.
Unusual Bleeding or Spotting
Any postmenopausal bleeding should trigger a prompt medical evaluation. While most cases are due to atrophic vaginitis or polyps, endometriosis lesions near the uterus can bleed intermittently, especially after hormonal therapy.
Related Symptom Groups
Perimenopause and Endometriosis Pain
The transition into menopause (perimenopause) often brings hormonal rollercoasters. For women with existing endometriosis, this can mean a flareup of pain that feels more intense than before. The key is recognizing that the pain isnt just hormones acting upit might be tissue reacting to those fluctuations.
Bowel Endometriosis After Menopause What to Notice
Look for persistent rectal pain, mucus discharge, or a feeling that you cant completely empty your bowels. These are not typical menopause complaints and warrant a pelvic MRI.
Bladder Endometriosis After Menopause Key Cues
Sudden urgency, a burning sensation when you pee, or pain that eases after emptying the bladderif antibiotics dont fix it, ask your doctor about a possible bladder lesion.
Endometriosis After Hysterectomy & Menopause
Even after a hysterectomy (removal of the uterus), endometrial tissue can persist on the ovaries, bowel, or pelvic sidewalls. Studies show that up to 5% of women develop new lesions after the surgery, especially if the ovaries are left intact.
Risk Enhancers
- Longterm HRT, especially estrogenonly formulations.
- Obesity, which can increase peripheral estrogen production.
- Family history of endometriosis or related autoimmune conditions.
How Diagnosis Works
When to See a Specialist
If youve got any of the redflag symptoms mentioned aboveespecially painful urination, unexplained bleeding, or severe pelvic painits time to book an appointment with a gynecologiconcologist or a pelvic pain clinic. Early assessment can spare you months of uncertainty.
Imaging Options
Transvaginal Ultrasound is often the first step; it can spot ovarian cysts or deep nodules. MRI provides a clearer picture of deep infiltrating disease, especially in the bowel or bladder. According to a 2023 review in , MRI boasts a sensitivity of over 90% for detecting bowel endometriosis.
Laparoscopy The Gold Standard?
When imaging isnt conclusive, a minimally invasive laparoscopy can both confirm the diagnosis and allow for immediate removal of lesions. Even in postmenopausal women, surgeons can safely perform this procedure, though theyll weigh the risks of anesthesia against the benefits.
Lab Work & Biomarkers
Blood tests such as CA125 can be elevated in endometriosis, but theyre not specific. Hormonal panels can help distinguish menopauserelated changes from disease activity.
Differential Diagnosis Checklist
Because many symptoms overlap with other conditions, a good clinician will rule out:
- Irritable Bowel Syndrome (IBS)
- Urinary Tract Infection (UTI) or Interstitial Cystitis
- Ovarian cysts or malignancy
- Atrophic vaginitis
Treatment Options Explained
Medical Therapy
Progestins (e.g., dienogest) can suppress any residual endometrial activity without the boneloss risks of GnRH analogues. GnRH analogues create a temporary menopauselike state, but theyre usually reserved for severe cases because they can worsen bone density.
For women on HRT, a lowdose combined regimen (estrogen+progestin) may keep hot flashes in check while limiting lesion growth. A comparison table can help you decide:
| Medication | How It Works | Pros | Cons |
|---|---|---|---|
| Progestin (dienogest) | Blocks estrogen receptors in lesions | Effective, oral, preserves bone | Weight gain, mood changes in some |
| GnRH analogue | Suppresses ovarian estrogen production | Strong lesion shrinkage | Hot flashes, bone loss needs addback therapy |
| Lowdose HRT (E+P) | Replaces estrogen while protecting uterus | Relieves menopausal symptoms | Potential lesion stimulation if not balanced |
Surgical Management
When medication isnt enough, surgeons may opt for laparoscopic removal of deep lesions. In postmenopausal patients, the goal is often symptom relief rather than fertility preservation. Recovery time is usually a few weeks, and many women report longlasting pain reduction.
Emerging Therapies
Aromatase inhibitors (like letrozole) are being tested for postmenopausal endometriosis because they block estrogen production in peripheral tissues. Meanwhile, selective progesterone receptor modulators (SPRMs) show promise in early trials. If youre curious, check the latest listings on for ongoing studies.
Managing SideEffects & QualityofLife
Any hormonal suppression can affect bone health and cardiovascular risk. Pairing treatment with calcium, vitamin D, and regular weightbearing exercise (think brisk walks or gentle yoga) helps keep your skeleton strong. Dont forget routine bonedensity scans if youre on GnRH analogues for more than six months.
Lifestyle SelfCare Tips
AntiInflammatory Nutrition
Foods rich in omega3s (salmon, walnuts, flaxseeds) can calm inflammation. Swap refined carbs for whole grains, and sprinkle turmeric or ginger into soups for an extra soothing kick.
Physical Activity & Pelvic Floor Therapy
Lowimpact cardiolike swimming or brisk walkingkeeps circulation moving without jarring joints. Adding pelvicfloor physiotherapy can release tension around the uterus and bladder, often easing pain more than medication alone.
StressReduction Techniques
Mindfulness meditation, deepbreathing exercises, or even a short daily gratitude journal can lower cortisol, which in turn may reduce pain perception. Ive found that a tenminute body scan before bed makes my nighttime cramps less intense.
Sleep Hygiene for Menopausal Pain
Keep your bedroom cool, limit screen time an hour before sleep, and consider a lavender pillow spray. Good sleep isnt just restorativeit can significantly blunt the intensity of pelvic pain.
Support Networks
Connecting with others who get it can be a lifesaver. Communities like or local endometriosis support groups offer shared stories, coping strategies, and a space to vent without judgment.
Final Takeaways Summary
To wrap it up, menopause endometriosis symptoms are real, varied, and often hide behind typical menopausal complaints. Recognizing the key warning signspersistent pelvic pain, bowel or bladder changes, unexplained bleeding, and atypical hot flashescan prompt timely evaluation.
Diagnosis blends smart imaging, careful lab work, and sometimes laparoscopy, while treatment blends medical therapy, possible surgery, and lifestyle adjustments. The best approach is personalized: a trusted specialist, a clear discussion of risks and benefits, and a supportive selfcare routine.
Dont let fear or misinformation keep you in the dark. If any of the symptoms resonated with you, consider reaching out to a pelvicpain specialist soon. And remember, youre not alonetheres a whole community ready to share, listen, and lift each other up.
Whats your experience with menopause and lingering pelvic pain? Share your story in the comments, ask questions, or simply let us know youre not navigating this alone. Were all in this together.
FAQs
Can endometriosis cause pain after menopause?
Yes. Even when estrogen levels fall, residual endometrial tissue can stay active or reactivate, leading to persistent pelvic or abdominal pain.
What urinary symptoms might indicate menopause endometriosis?
Frequent urgency, painful urination, or occasional blood in the urine that does not improve with standard antibiotics can be a sign of bladder endometriosis.
How is bowel endometriosis distinguished from IBS in post‑menopausal women?
Bowel endometriosis often presents with rectal bleeding, pain that worsens during intercourse, and lesions visible on MRI, whereas IBS symptoms are usually linked to meals or stress and have normal imaging.
Are hormone replacement therapies safe for women with lingering endometriosis?
Combined low‑dose estrogen‑plus‑progestin HRT can relieve menopausal signs while minimizing lesion stimulation, but estrogen‑only regimens may exacerbate endometriosis growth.
What treatment options are most effective for menopause endometriosis symptoms?
Medical options include progestins (e.g., dienogest) and, in severe cases, GnRH analogues with add‑back therapy. Surgical removal via laparoscopy is considered when medication fails, and emerging therapies like aromatase inhibitors are being studied.