Got the news that you have a prepyloric ulcer and wondering how to get back to feeling normal? The quickest path to healing usually starts with a mix of acidblocking medication, testing (and treating) for H.pylori, and a few lifestyle tweaks. In the next few minutes well walk through the warning signs, why the ulcer shows up right before the pylorus, and the proven treatment plan doctors trust all while keeping the pros and cons frontandcenter.
Stick around, because youll leave with a clear, stepbystep roadmap, a handy symptom checklist, and the confidence to talk with your doctor about the best plan for you.
Prepyloric Ulcer Basics
What exactly is a prepyloric ulcer?
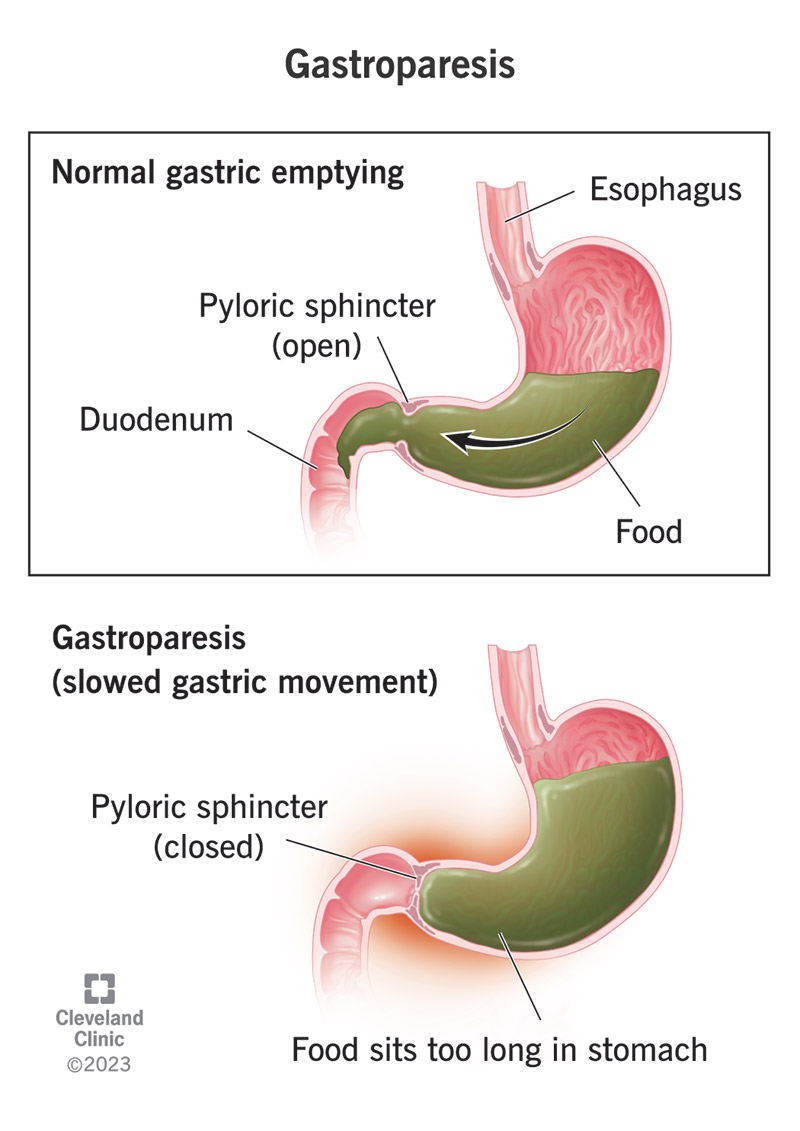
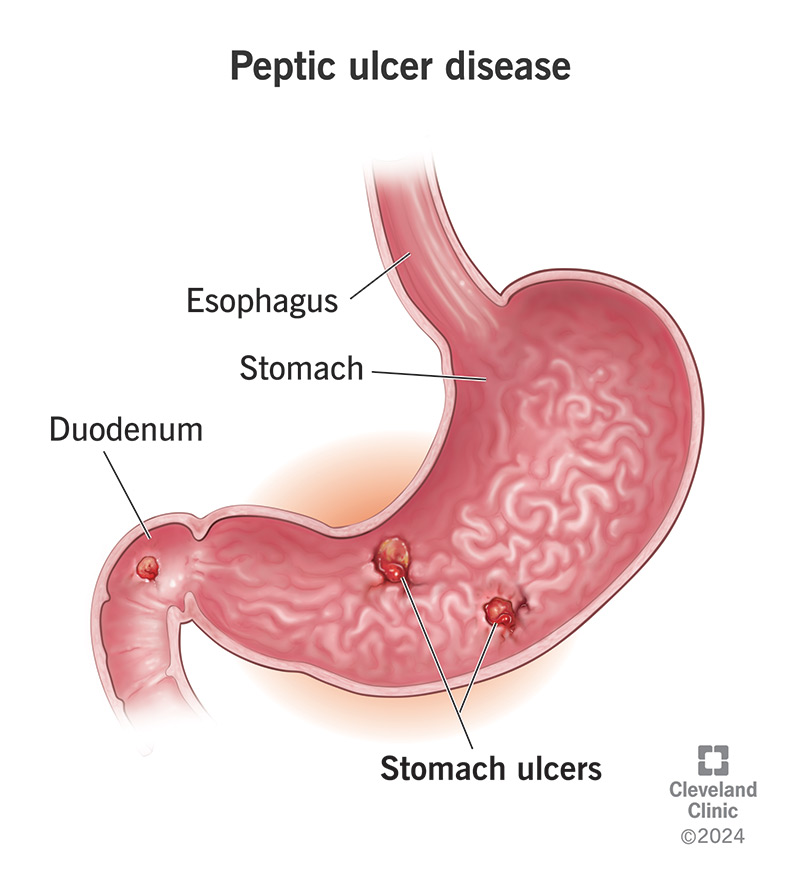
The prepyloric region is the stretch of stomach tissue just before the pyloric sphincter the gateway that releases stomach contents into the duodenum. When the lining there gets eroded, you end up with a prepyloric ulcer, a type of peptic ulcer that sits in that narrow zone.
Typical prepyloric ulcer symptoms
Symptoms can feel like a lowgrade alarm or a fullblown panic attack, depending on the ulcers size. Common clues include:
- Burning or gnawing pain that often improves after eating (but can flare up a few hours later)
- Nausea or a feeling of fullness even after a tiny meal
- Early satiety you get full after just a few bites
- Unexplained weight loss or loss of appetite
- Occasional vomiting of blood or coffeegroundlike material (a redflag sign that needs urgent care)
What triggers a prepyloric ulcer?
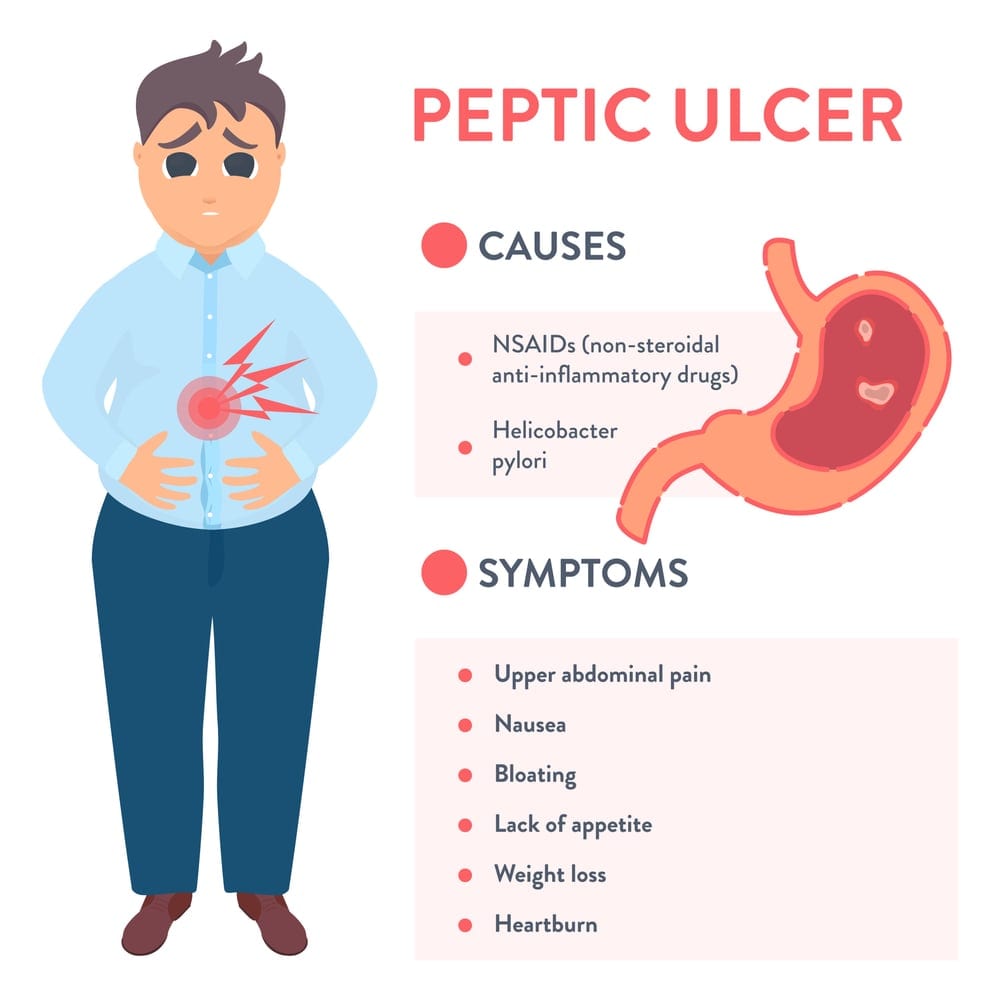
Most ulcers have a couple of usual suspects:
- H.pylori infection the bacteria that love the stomach lining.
- Regular use of nonsteroidal antiinflammatory drugs (NSAIDs) like ibuprofen or aspirin.
- Smoking, excessive alcohol, and chronic stress, which all boost stomach acid.
- Rarely, conditions like ZollingerEllison syndrome that crank up acid production.
According to , combining these factors can make the prepyloric region especially vulnerable because its blood supply is a bit more limited than other stomach areas.
How Is It Diagnosed?
Endoscopy the gold standard
The most reliable way to confirm a prepyloric ulcer is through a prepyloric stomach endoscopy. A thin, flexible camera slips down your throat, letting the doctor see the ulcer directly and take a tiny biopsy if needed. Its quick, usually done under mild sedation, and gives a clear picture of the ulcers size and depth.
Noninvasive tests for H.pylori
If youve got symptoms, your doctor may also order a urea breath test or a stool antigen test. These are painless and can tell you whether H.pylori is part of the problem a key piece of the treatment puzzle.
ICD10 coding what clinicians use
In medical records, prepyloric ulcers are logged under the code K27.0 Prepyloric ulcer. Knowing this code helps when youre dealing with insurance or looking up research data.
Preparing for your endoscopy
- Fast for at least 6 hours before the procedure.
- Tell your doctor about any medications, especially blood thinners or NSAIDs.
- Bring a list of current meds and any allergies.
Treatment Options Overview
Firstline medications
The cornerstone of ulcer healing is to reduce stomach acid so the tissue can repair itself.
- Protonpump inhibitors (PPIs) drugs like omeprazole, esomeprazole, and lansoprazole are the most potent acid suppressors. A study from showed PPIs close 90% of prepyloric ulcers within 8weeks.
- H2blockers ranitidine or famotidine can work, but theyre generally less effective for prepyloric ulcers, which tend to be more resistant (see a ).
Eradicating H.pylori
If the breath test is positive, the usual approach is triple therapy: two antibiotics (often clarithromycin and amoxicillin) plus a PPI for 14 days. According to , this combo clears the infection in about 8090% of cases.
Protective agents & adjuncts
- Sucralfate a coating that shields the ulcer from acid. A found sucralfate as effective as cimetidine for ulcer healing, with fewer sideeffects.
- Bismuth subsalicylate often added to quadruple therapy when antibiotic resistance is a concern.
Lifestyle & diet tweaks the fastest way to boost healing
Even the strongest meds need a supportive environment. Try these:
- Stop NSAIDs (switch to acetaminophen for pain).
- Quit smoking nicotine impairs ulcer healing.
- Limit alcohol and caffeine, which can increase acid.
- Eat small, frequent meals instead of big, heavy ones.
- Avoid spicy, acidic, or fried foods that irritate the stomach lining.
These changes arent just nice to have they can cut healing time by a week or more according to clinical observations.
Medication Comparison Table
| Drug Type | Onset of Relief | Success Rate (812weeks) | Common Sideeffects |
|---|---|---|---|
| PPIs (Omeprazole, Esomeprazole) | Within 2448hours | 90% | Headache, mild diarrhea |
| H2Blockers (Ranitidine, Famotidine) | 23days | 60% (lower in prepyloric) | Rare dizziness, fatigue |
| Sucralfate | 34days | 80% | Constipation, rare allergic rash |
When Treatment Fails
Spotting resistant ulcers
If youve been on a full dose of a PPI for 812weeks and still feel that burning, its time to reassess. Persistent pain, bleeding, or a ulcer that hasnt shrunk on repeat endoscopy signals treatmentresistant disease.
Secondline strategies
- Increase the PPI dose (double the standard amount) or switch to a different PPI.
- Add sucralfate to the regimen for an extra protective coat.
- Consider bismuthbased quadruple therapy if antibiotic resistance is suspected.
Surgical options a last resort
Rarely, a prepyloric ulcer can perforate or cause uncontrolled bleeding. In those cases, a surgeon may perform a partial gastrectomy or a more focused repair of the prepyloric region. notes that surgery carries risks like infection, nutritional deficiencies, and a recovery period of 46 weeks, so its only considered when medical therapy truly fails.
Realworld case
John, a 48yearold accountant, went to the ER with severe upperabdominal pain. Endoscopy showed a 1cm prepyloric ulcer that hadnt healed after 10weeks of standard PPIs. His doctor switched him to highdose esomeprazole plus sucralfate and added a 2week course of bismuth quadruple therapy. Six weeks later, the ulcer had vanished, and his pain was gone. Stories like Johns illustrate how a tailored, aggressive approach can rescue a stubborn ulcer.
Benefits and Risks
What you gain
- Rapid symptom relief (often within days of starting a PPI).
- High likelihood of complete healing (90%+ with proper regimen).
- Reduced risk of serious complications like bleeding or perforation.
Potential downsides
- Longterm PPI use may be linked to vitamin B12 deficiency, magnesium loss, and increased infection risk so doctors aim for the shortest effective course.
- Antibiotic resistance can make the H.pylori regimen less successful, requiring alternative drugs.
- Surgery, while rare, carries the usual operative risks and a need for dietary adjustments afterward.
Finding the right balance
Think of ulcer treatment like tuning a guitar. You need the right tension (acid suppression) and the proper strings (antibiotics, protective agents) to play a harmonious tune. Too much tension can snap the strings (sideeffects), while too little leaves the music out of tune (persistent pain). Working closely with your gastroenterologist ensures you strike that perfect chord.
Bottom Line: Your Path to Healing
If youve just learned you have a prepyloric ulcer, dont panic. Start with a prescribed PPI, get tested for H.pylori, and adopt a few friendly lifestyle tweaks. Keep an eye on your symptoms, and if things dont improve within a couple of months, bring it up with your doctor theyll know when to intensify therapy or consider a secondline plan.
Healing is a partnership between you, your doctor, and the medications that protect your stomach lining. By staying informed and proactive, youll give your body the best chance to repair, recover, and get back to enjoying meals without that unsettling gnaw.
Whats your experience with stomach ulcers? Share your story in the comments, ask any lingering questions, or download our free symptomtracker checklist to stay on top of your progress. Were all in this together.
For a concise patient guide on peptic ulcer symptoms and causes, see the Mayo Clinic overview: peptic ulcer symptoms and causes.
FAQs
What causes a prepyloric ulcer?
Most prepyloric ulcers develop from infection with Helicobacter pylori, regular NSAID use, smoking, excessive alcohol, or conditions that increase stomach acid such as Zollinger‑Ellison syndrome.
How is a prepyloric ulcer diagnosed?
The gold‑standard test is an upper endoscopy, which lets the doctor view the ulcer directly and take biopsies if needed. Non‑invasive H. pylori tests (urea breath or stool antigen) are also used.
What are the first‑line medications for prepyloric ulcer treatment?
Proton‑pump inhibitors (e.g., omeprazole, esomeprazole) are the most effective acid‑suppressing drugs. If H. pylori is present, a 14‑day triple therapy (two antibiotics plus a PPI) is standard.
When should I consider second‑line therapy or surgery?
If symptoms persist after 8‑12 weeks of full‑dose PPI therapy, or if the ulcer shows no healing on repeat endoscopy, doctors may increase the PPI dose, add sucralfate or bismuth‑based quadruple therapy, and, in rare cases of perforation or uncontrolled bleeding, surgical repair.
Can lifestyle changes speed up healing of a prepyloric ulcer?
Yes. Stopping NSAIDs, quitting smoking, limiting alcohol and caffeine, eating small frequent meals, and avoiding spicy or fried foods can shorten healing time by a week or more and improve overall treatment success.