Most people dont realize that a leukemia that starts in the blood can quietly migrate to the brain and spinal cord. In adult Bcell acute lymphoblastic leukemia (ALL) this happens in410% of cases, showing up as headaches, vision changes, or even seizures.
Why does this matter? Because once the cancer reaches the central nervous system (CNS) the treatment plan shifts, the sideeffects change, and the outlook can look a bit different. Knowing the signs, the tests, and the options lets you (or a loved one) stay a step ahead and make informed choices with your doctor.
What is CNS involvement
Definition
CNS involvement simply means that leukemic blasts have infiltrated the meningesthe protective layers surrounding the brain and spinal cord. In Bcell ALL this is called meningeal disease and is diagnosed when cancer cells are found in the cerebrospinal fluid (CSF) or on MRI.
Incidence & epidemiology
Recent studies show that about 512% of newly diagnosed adult Bcell ALL patients have CNS disease at presentation, while up to 20% can develop it later during treatment. The risk climbs a bit higher in the mature Bcell subtype and when certain cytogenetic abnormalities are present.
Why Bcell subtype matters
The Bcell lineage seems to have a slightly higher affinity for the CNS niche compared with Tcell ALL. Researchers think this is linked to surface receptors that help blasts cross the bloodbrain barrier. In practice, it means we keep a closer eye on patients with Bcell ALL when were planning CNS prophylaxis.
Pathophysiology basics
Leukemic cells travel through the bloodstream, slip past the bloodbrain barrier, and lodge in the leptomeninges. Once there, they can multiply in the CSF, creating a reservoir thats shielded from many systemic chemotherapy agentshence the need for intrathecal (directly into the CSF) treatment.
How does it present
Typical symptoms
Symptoms can be subtle at first. Common cues include:
- Persistent headache that doesnt improve with usual pain relievers
- Neck stiffness or a feeling of pressure around the head
- Blurred vision or double vision
- Facial droop, slurred speech, or other cranial nerve palsies
- Seizures, especially in someone without a prior seizure history
- Sudden changes in mental status, like confusion or drowsiness
All CNS involvement symptoms vs. systemic signs
Its easy to mix CNS clues with the usual ALL complaints (fatigue, fever, bone pain). The key difference is that CNSrelated symptoms involve the nervous systemyoull feel them in your head, eyes, or muscles, not just in your blood counts.
When symptoms appear
Some patients notice these signs right at diagnosis, but many develop them later, often after the first few cycles of chemotherapy when the disease hides in the CSF. The median time to CNS relapse is around 812months postinduction, though it can be sooner in highrisk groups.
Diagnostic clues on exam
On a quick neurological exam you might pick up:
- Positive Kernig or Brudzinski signs (suggesting meningeal irritation)
- Weakness in a specific cranial nerve distribution
- Abnormal pupillary reflexes
Realworld vignette
Take Maya, a 38yearold accountant who was diagnosed with Bcell ALL six months ago. She finished her first induction and felt greatuntil she started getting pressure headaches that lingered for days. A quick lumbar puncture revealed a handful of blasts in her CSF, confirming CNS involvement. Early detection let her team switch to a more aggressive intrathecal regimen, and shes now in remission.
How is it diagnosed
Lumbar puncture basics
The gold standard is a lumbar puncture (LP). Youll have a small needle inserted between the lower back vertebrae, and about 610mL of CSF is collected. The fluid is then examined under the microscope, and often sent for flow cytometry.
Flow cytometry vs. cytology
Traditional cytology catches about 30% of cases, while flow cytometry bumps that up to roughly 70%. The more sensitive technique looks for cell surface markers specific to Bcell blasts, giving a clearer picture of CNS disease.
Imaging role
MRI of the brain (with contrast) and spine can show meningeal enhancement or tiny leptomeningeal nodules. Its especially useful when the CSF is negative but symptoms persist.
CNS2 vs. CNS3 classification
Doctors classify CNS disease into three groups:
- CNS1: No blasts in CSF, count5cells/L.
- CNS2: Blasts present but 5cells/L or cytology+no neurological signs.
- CNS3: 5cells/L with blasts, or any neurologic manifestation.
CNS3 carries the highest risk and typically triggers more intensive therapy.
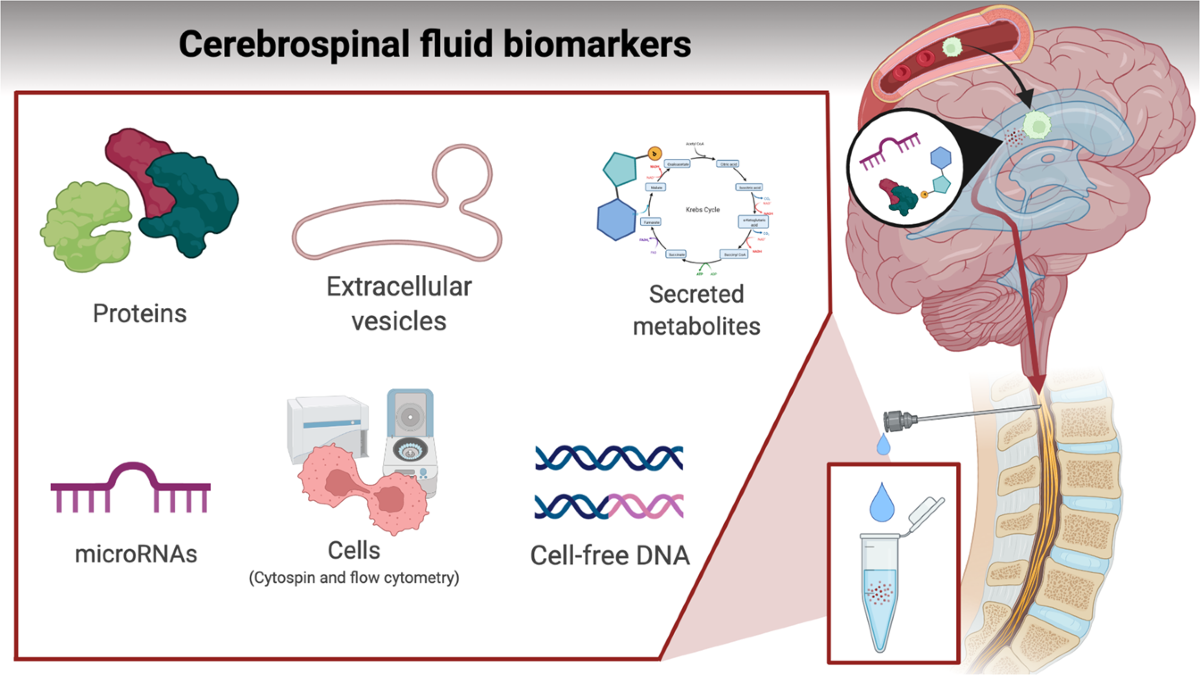
Emerging biomarkers
Scientists are testing cellfree DNA from CSF and nextgeneration sequencing panels to catch disease even earlier. These methods arent standard yet, but theyre promising for future liquid biopsy monitoring.
Stepbystep LP protocol (table)
| Step | Details |
|---|---|
| 1. Preparation | Patient lies on side, knees drawn to chest; sterile drape applied. |
| 2. Needle selection | 22gauge atraumatic needle reduces postLP headache risk. |
| 3. Sample volume | Collect 610mL; split into tubes for cytology, flow, culture. |
| 4. Handling | Keep specimens on ice, process within 30minutes for optimal flow results. |
Treatment options
Standard frontline therapy
Most patients receive a combination of systemic highdose chemotherapy plus intrathecal (IT) methotrexate or cytarabine. IT therapy is given on a scheduleoften on days1,8,15 of each cycledirectly targeting the CSF sanctuary.
CNSdirected radiation
Wholebrain or craniospinal radiation is reserved for those who dont clear blasts after IT chemo or who have CNS3 disease. While effective, it carries longterm risks like memory problems and secondary malignancies, so doctors weigh benefits carefully.
Targeted & cellular therapies
CART cells, especially CD19directed products like brexucabtagene autoleucel, have shown activity in the CNS because the engineered Tcells can cross the bloodbrain barrier. A 2023 study reported a 70% CNS remission rate in relapsed patients, though close monitoring for neurotoxicity is essential ().
Relapse management
If disease returns in the CNS, options include:
- Reinduction with intensified IT methotrexate plus highdose systemic chemo.
- Allogeneic stemcell transplantoften the only curative intent for highrisk CNSpositive patients.
- Novel agents such as blinatumomab (a bispecific Tcell engager) that can be administered intravenously yet still achieve CSF penetration.
Supportive care & monitoring
Because the CNS is a delicate area, we keep an eye on neurocognitive function, manage seizures with prophylactic antiepileptics when needed, and repeat CSF analysis every 12months during the first year of therapy.
ProsCons table
| Therapy | Benefits | Risks |
|---|---|---|
| Intrathecal methotrexate | High local control; widely available | Arachnoiditis, chemical meningitis |
| Cranial radiation | Rapid clearance of bulk disease | Neurocognitive decline, secondary tumors |
| CART (CD19) | Targets hidden blasts; durable remission | Cytokine release syndrome, neurotoxicity |
| Allogeneic transplant | Potential cure for highrisk patients | Graftversushost disease, infections |
Prognosis and survival
Overall survival difference
Patients with CNSpositive Bcell ALL typically have a 5year overall survival (OS) that is 1015% lower than those without CNS disease. In a multicenter cohort of 1,200 adults, CNS3 patients had a 3year OS of 42% versus 57% for CNS1 ().
Factors that improve prognosis
Good prognostic signs include:
- Early clearance of blasts from CSF after the first few IT doses.
- Younger age (<60years) and good performance status.
- Favorable cytogenetics such as ETV6RUNX1.
- Incorporation of CART or blinatumomab in consolidation.
Impact of CNS relapse
A CNS relapse often signals a more aggressive disease biology. Median survival after a CNSonly relapse drops to around 1218months unless a transplant or CART is pursued.
Longterm neurocognitive outcomes
Even when the cancer is cleared, some survivors report memory lapses, attention issues, or reduced processing speedparticularly if they received cranial irradiation. Ongoing neurorehab and cognitive testing can help mitigate these effects.
Riskstratification table
| Risk Level | Key Features | Suggested Approach |
|---|---|---|
| Low | CNS1, age <45, favorable genetics | Standard IT prophylaxis, no radiation |
| Intermediate | CNS2, age 4560, mixed genetics | Intensified IT schedule, consider early CART |
| High | CNS3, any age with adverse cytogenetics | IT + radiation + possible transplant or CART |
Practical tips you can use today
Symptom checklist (downloadable)
If you or a loved one is undergoing treatment for Bcell ALL, keep a simple list handy:
- New or worsening headache?
- Neck stiffness or pressure feeling?
- Vision changes (blurred, double, loss of peripheral vision)?
- Facial droop, slurred speech, or trouble swallowing?
- Any seizure activity, even a brief blank stare?
Jot down the date, severity, and any triggers, then share it with your oncology team right away.
When to ask for a lumbar puncture
If you notice any of the above symptoms persisting for more than 48hours, request a repeat CSF analysis. Early detection is the difference between a short IT boost and a more intensive treatment course.
How to talk to your doctor
Bring up three key points during your appointment:
- Ive been experiencing X symptom; could this be CNS involvement?
- What is my current CNS status (CNS1/2/3) and how does that affect my treatment plan?
- Are there clinical trials or newer therapies like CART that might be suitable for me?
Resources you can trust
For deeper guidelines, the provide uptodate recommendations on CNS prophylaxis and relapse management. Keep a copy bookmarked for reference during clinic visits.
Conclusion
Understanding Bcell ALL CNS involvement isnt just academicits a lifesaver. The disease may be rare, but its impact is real: headaches can be the first whisper of cancer hiding in the brain, and the right tests can catch it before it spreads further. Modern toolsintrathecal chemotherapy, targeted CART cells, and careful imaginggive us a fighting chance, even though the prognosis still lags behind CNSnegative cases.
Stay proactive, keep a symptom diary, and never hesitate to ask your doctor for a CSF check if something feels off. Knowledge, early detection, and an open dialogue with your care team are the best weapons you have.
If youve been through this journey or are currently navigating it, Id love to hear how youre managing the challenges. Together we can turn the scary medical jargon into something we all understand and conquer.
For patients also managing other cancer concerns, dietary and supportive measures may help with overall wellbeing see guidance on a Cancer diet plan that can complement medical treatment.
FAQs
What does CNS involvement mean in B-cell ALL?
CNS involvement in B-cell ALL refers to the infiltration of leukemic blasts into the meninges and cerebrospinal fluid, indicating leukemia cells have spread to the brain or spinal cord.
How common is CNS involvement in adult B-cell ALL?
About 5-12% of adults with newly diagnosed B-cell ALL have CNS disease at diagnosis, and up to 20% may develop CNS involvement during treatment.
What are the typical symptoms of CNS involvement in B-cell ALL?
Symptoms include persistent headaches, neck stiffness, vision changes, facial weakness, seizures, and altered mental status, which differ from systemic leukemia symptoms.
How is CNS involvement diagnosed in B-cell ALL?
The gold standard diagnosis is a lumbar puncture to analyze cerebrospinal fluid with cytology and flow cytometry, supported by MRI imaging when necessary.
What treatment options are available for CNS involvement in B-cell ALL?
Treatment typically involves systemic chemotherapy combined with intrathecal chemotherapy; radiation and CAR T cell therapies are considered for resistant or high-risk cases.