If you're living with ulcerative colitis (UC), the thought that it might someday turn into colon cancer can feel like a heavy cloud hanging over everyday life. The good news? It's not a certainty, and there are concrete steps you can take to keep that risk as low as possible.
In the next few minutes we'll untangle the science, flag the warning signs, and lay out a clear plan you can follow. Think of this as a friendly chat over coffeeno jargon, just the facts you need to feel empowered.
Why Risk Increases
What makes inflammation a cancer catalyst?
Chronic inflammation is like a tiny, relentless fire that never fully goes out. In UC, the colon's lining is constantly irritated, forcing the cells to divide and repair over and over. Each division carries a chance of a DNA mistake, and over years those tiny errors can stack up into dysplasiaa precancerous change.
Researchers have traced this pathway in detail. According to a study published in Gastroenterology, patients with longstanding UC show a sixfold increase in the molecular markers linked to colorectal cancer.
How big is the risk, really?
Numbers can feel cold, but they give us a reality check. After 10 years of UC, roughly 2% of patients develop colon cancer; after 20 years, that rises to around 8%. For the average person, the lifetime risk sits near 1%. So while UC does boost the odds, most people never cross that line.
Good news: advances in medication and regular colonoscopic surveillance have begun to nudge those percentages down. A 2019 Lancet review noted a modest but steady decline in cancer rates among patients on modern biologics.
Who's Most at Risk
Does disease extent matter?
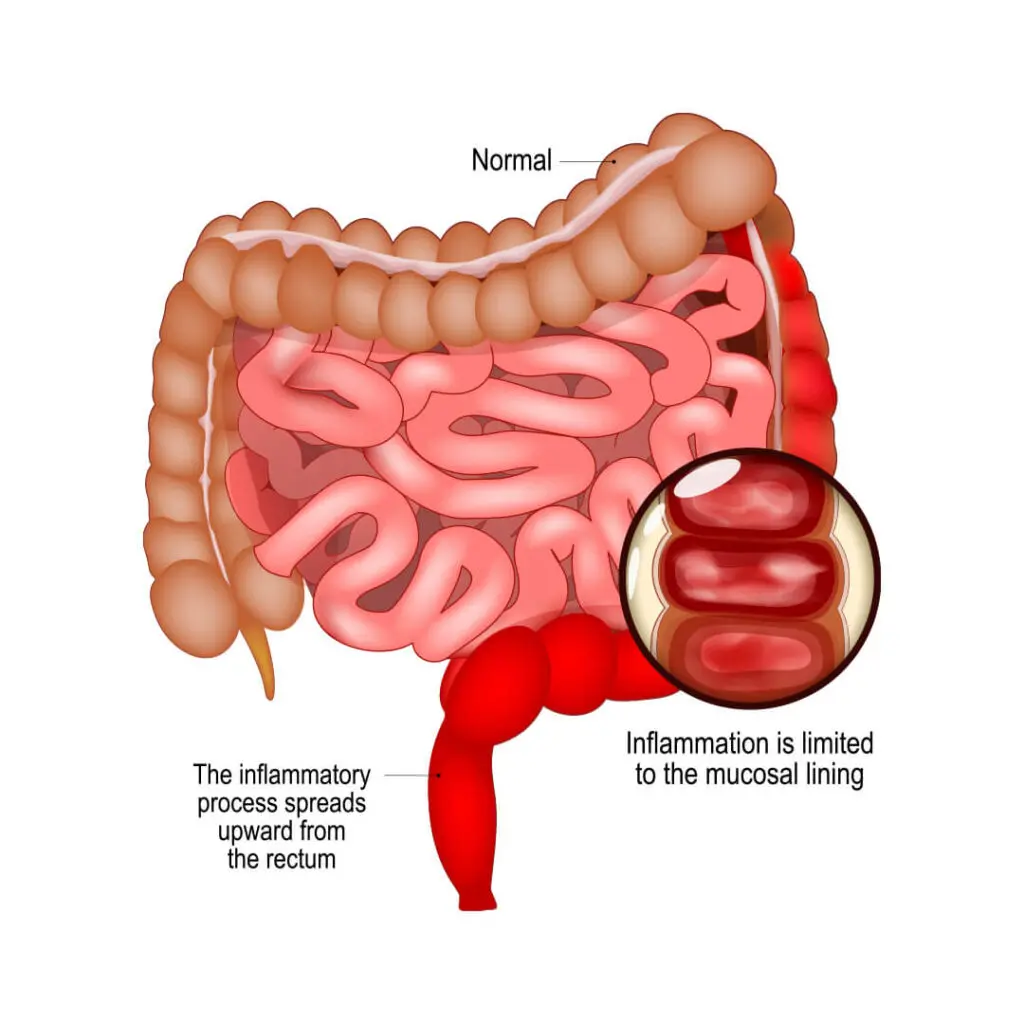
Yes. Left-sided ulcerative colitiswhere inflammation spreads up to the splenic flexurecarries a higher cancer risk than proctitis (inflammation limited to the rectum). Pancolitis, affecting the entire colon, tops the risk chart.
Beyond the colon: other red flags
Things like primary sclerosing cholangitis (PSC), a liver condition that often coexists with UC, can triple your cancer odds. A family history of colorectal cancer, smoking, and even certain genetic markers add extra layers of risk.
What percentage actually develop cancer?
| Duration of UC | Approximate Cancer Risk |
|---|---|
| 5 years | 0.5% |
| 10 years | 2% |
| 15 years | 5% |
| 20+ years | 8% |
These figures come from large cohort studies pooled by the Crohn's & Colitis Foundation.
Spotting Warning Signs
How do UC symptoms differ from early cancer signs?
Both conditions can cause blood in the stool and abdominal cramping, which makes it tricky. The key is to watch for changes:
- New or worsening anemia despite staying on your usual meds.
- Sudden change in stool caliberthinner than usual.
- Persistent fatigue that doesn't improve with rest.
- Unexplained weight loss over a few weeks.
Here's a quick comparison table you can keep handy:
| Symptom | Typical UC Flare | Possible Cancer Indicator |
|---|---|---|
| Blood in stool | Common, often with mucus | Can appear, but look for persistence |
| Abdominal pain | Crampy, relieved after bowel movement | Persistent, unrelated to eating |
| Weight loss | Rare, usually due to flare diet | Unintended, steady loss |
| Stool shape | Varies, usually normal caliber | Thin "pencil-thin" stools |
When to call your doctor
Any of those red-flag symptoms persisting for more than two weeks should prompt a prompt colonoscopy. It's better to get a "nothing to see here" result than to wait until the next routine checkup.
Timeline to Cancer
How long does it usually take?
On average, dysplasia can develop into invasive cancer in about 812 years for patients with extensive disease. Some cases accelerate if inflammation remains uncontrolled, while others remain stable for decades.
What speeds the progression?
Frequent flare-ups, poor adherence to maintenance medication, and missed surveillance colonoscopies are the biggest accelerators. Think of them as neglected potholes that eventually cause a crash.
Surveillance Strategies
What's the ideal colonoscopy schedule?
The American Gastroenterological Association recommends a colonoscopy every 13 years once you've had UC for 810 years, especially if you have extensive or left-sided disease.
Can newer techniques help?
Yes! Chromoendoscopyspraying a dye during colonoscopyhighlights subtle dysplastic patches that standard scopes might miss. Biomarkers like p53 or Ki67 staining are also emerging tools, though they're still largely research-phase.
When to see a specialist
If dysplasia is found, a high-volume IBD center can guide you through options like endoscopic resection versus surgery. Their expertise often translates into better outcomes and less aggressive surgery.
Treatment Options
If cancer is diagnosed, what are the choices?
Surgery is the cornerstone. A total colectomy removes the entire colon and eliminates the cancer risk, but it's a big step. In select cases with early-stage disease, a segmental resection (removing only the affected part) may be possible.
Chemotherapy regimens such as FOLFOX or FOLFIRI are standard for stage III/IV disease. For tumors that are MSI-high (a genetic feature), immunotherapy with pembrolizumab has shown impressive responses.
Clinical trials are worth exploring. The National Cancer Institute continually runs studies on novel targeted therapies and vaccine-based approaches for colorectal cancer arising from IBD.
Lifestyle Management
How can daily habits lower risk?
Sticking to your maintenance medswhether 5-ASA, vedolizumab, or infliximabhas been shown to cut cancer risk by up to 50%.
Diet matters too. A Mediterranean-style diet rich in fiber, omega-3 fatty acids, and antioxidants can calm inflammation. Regular exercise (at least 150 minutes of moderate activity per week) improves gut motility and overall immune health.
And yes, quitting smoking is a must. Smokers with UC have not only higher flare rates but also a steeper cancer curve.
Why mental health counts
Stress can flare UC, and flares can make you feel helpless. Joining a support group or seeing a therapist can improve medication adherence and overall quality of lifeboth indirect shields against cancer.
UC vs Crohn's Risk
How do the two IBDs compare?
Both ulcerative colitis and Crohn's disease increase colorectal cancer risk, but UC carries a slightly higher odds ratio. Large-scale data suggest UC patients have about a 23 higher relative risk, while those with Crohn's limited to the colon see a 1.5 increase.
What does that mean for you?
If you have Crohn's disease affecting the colon, you still need regular surveillance, but the timeline may be a bit more forgiving. For UC, the emphasis on early and frequent colonoscopies is stronger.
Key Takeaways
1. Risk is real but manageableUnderstanding the numbers and staying on a tight surveillance schedule can catch dysplasia before it becomes cancer.
2. Listen to your bodyNew or worsening symptoms deserve a prompt checkup; don't wait for a routine appointment.
3. Proactive care winsOptimized medication, a balanced diet, regular exercise, and mental-health support dramatically lower the odds of cancer.
Take the next step today: schedule your next colonoscopy, talk to your gastroenterologist about the best maintenance therapy for you, and consider joining an IBD community for shared stories and encouragement.
Got questions or personal experiences you'd like to share? Drop a comment below or reach outyour journey can help someone else feel less alone.
FAQs
How often should I get a colonoscopy if I have ulcerative colitis?
Guidelines recommend a colonoscopy every 1‑3 years after 8–10 years of disease, especially for extensive or left‑sided colitis.
Can medication lower my ulcerative colitis colon cancer risk?
Yes. Maintenance therapies such as 5‑ASA, biologics (e.g., vedolizumab, infliximab) have been shown to reduce cancer risk by up to 50 %.
What are the early warning signs that ulcerative colitis might be turning into cancer?
Watch for new anemia, persistent thin or pencil‑shaped stools, unexplained weight loss, and fatigue lasting more than two weeks.
Is a Mediterranean diet helpful for reducing cancer risk?
A diet rich in fiber, omega‑3s, fruits, and vegetables can calm inflammation and is associated with a modest reduction in colorectal cancer risk.
How does having primary sclerosing cholangitis affect my cancer risk?
PSC triples the odds of developing colon cancer, so patients with both conditions need tighter surveillance—often annually.