What is RTA?
In a nutshell, renal tubular acidosis (RTA) is an acidbase disorder that crops up when the kidneys tiny tubes cant properly balance the bodys pH. Think of the kidneys as a coffeemaker that has to keep the brew just right; when the filter (the tubules) gets a bit wonky, the whole pot ends up too acidic.
RTA isnt just one disease its a family of conditions, each with its own location of defect and set of quirks. Understanding the renal tubular acidosis types is the first step toward getting the right treatment.
Main RTA Types
| Type | Where the defect lives | Key lab clues | Typical signs |
|---|---|---|---|
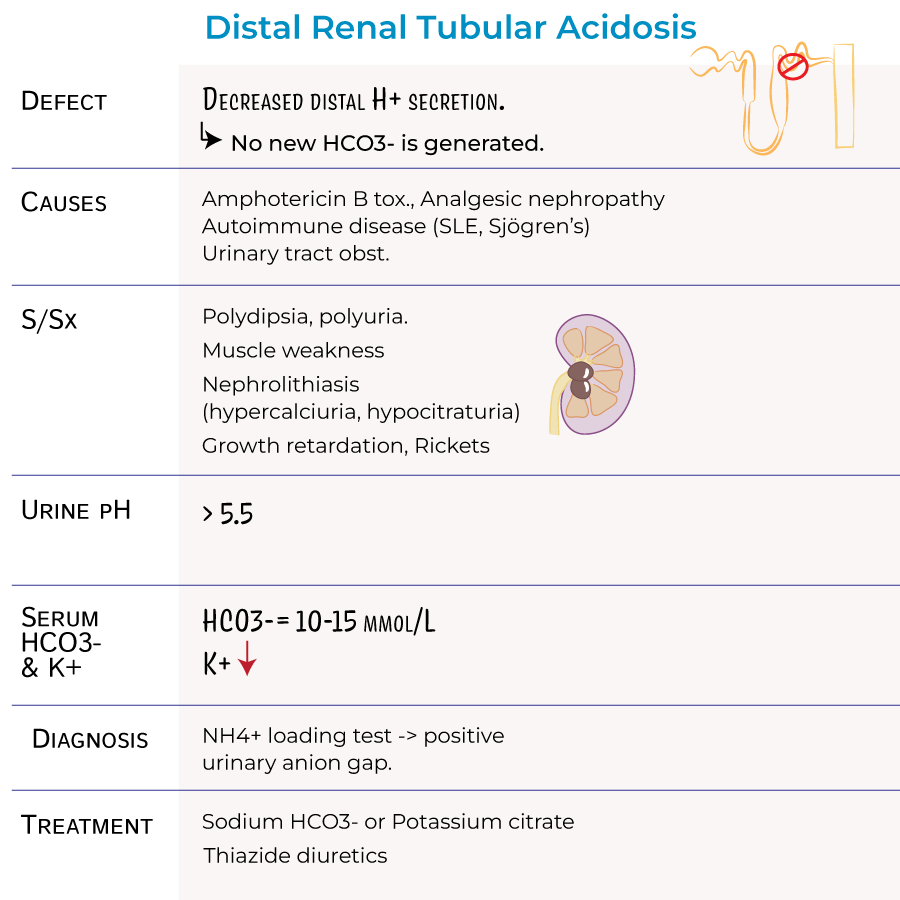
| Type1 Distal RTA | Distal tubule (impaired H secretion) | Low urine pH (<5.5), normal aniongap metabolic acidosis | Kidney stones, muscle weakness, growth delay (kids) |
| Type2 Proximal RTA | Proximal tubule (poor HCO reabsorption) | High urine HCO loss, variable urine pH | Bone pain, rickets/osteomalacia, polyuria |
| Type4 Hyperkalemic RTA | Collecting duct (aldosterone resistance) | HyperK, mild acidosis, urine pH usually >5.5 | Fatigue, hypertension, often linked to diabetes |
Why the type3 mystery?
Older textbooks sometimes list a type3 as a mix of distal and proximal defects. Modern guidelines (like those from the ) consider it extremely rare and usually just group those cases under type1 or type2. So, for most of us, focusing on types1,2, and4 does the trick.
Symptoms by Type
Distal (type1) clues
If youre hearing about kidney stones popping up out of nowhere, thats a red flag for distal RTA. Other hints include a persistent tiredmuscle feeling and, in kids, slower growth.
Proximal (type2) clues
Imagine constantly feeling achy, especially in your bones, and needing to pee a lot. Those are classic for proximal RTA, where the body loses bicarbonate and the skeleton tries to compensate.
Hyperkalemic (type4) clues
Type4 often sneaks in quietly. You might see a mild acidosis on lab work, higher potassium levels, and maybe an underlying condition like diabetic kidney disease. Symptoms can be vague fatigue, a little swelling, or high blood pressure.
Adults vs. kids
While kids usually reveal themselves through growth issues and bone problems, adults tend to notice symptoms in adults like kidney stones (type1) or unexplained muscle cramps (type2). The key is that the renal tubular acidosis symptoms vary, but the lab pattern stays consistent.
How RTA Is Diagnosed
Diagnosing RTA is a bit like detective work. You gather clues from blood, urine, and the patient\'s story, then match them to the renal tubular acidosis diagnosis criteria.
Core lab checklist
- Serum anion gap usually normal.
- Serum bicarbonate (HCO) low.
- Urine pH <5.5 for type1, >5.5 for type2 and4.
- Serum potassium normal/low in types12, high in type4.
Special tests
For type1, doctors may give an ammonium chloride challenge to see if the kidneys can acidify urine. For type2, they calculate the fractional excretion of bicarbonate. These arent routine, but theyre gold standards when the picture is blurry.
Decision flow
Think of it as a simple flowchart: start with low bicarbonate check urine pH look at potassium decide which type fits best. A quick visual can even snag a featured snippet in Google!
If you or your clinician are looking for practical management tips that overlap with other kidney problems (for example, medications and monitoring), see this brief guide on renal tubular acidosis treatment for specific dosing and followup ideas.
Treatment Options
General goals
Regardless of the type, we want to:
- Correct the acidosis.
- Prevent complications (stones, bone loss, cardiovascular issues).
- Balance electrolytes.
Type1 (Distal) care
Alkali therapy is the cornerstone. Sodium bicarbonate or potassium citrate is prescribed, often in divided doses. The citrate version helps prevent calcium stone formation a nice bonus.
Type2 (Proximal) care
Here you need larger doses of bicarbonate because the proximal tubule keeps spilling it. Patients are usually told to monitor their sodium intake, because highdose bicarbonate can add extra sodium.
Type4 (Hyperkalemic) care
First, address the aldosterone problem. Fludrocortisone can boost potassium excretion, and a lowpotassium diet helps. Treat the underlying disease for many, that means tight bloodsugar control in diabetes.
Medication snapshot
| Medication | Typical Dose | Key Monitoring | Possible Sideeffects |
|---|---|---|---|
| Sodium Bicarbonate | 0.51g 34/day | Serum HCO, blood pressure | Na overload, edema |
| Potassium Citrate | 1020mEq 23/day | Serum K, urine pH | GI upset, hyperK (rare) |
| Fludrocortisone | 0.050.2mg daily | BP, serum K, Na | Hypertension, edema |
Lifestyle tips
Stay wellhydrated, especially if youre prone to stones. For type2, calciumrich foods (like dairy) can help bone health, but keep an eye on sodium. And dont forget regular labs theyre the best way to adjust your meds before anything goes offtrack.
Balancing Risks & Benefits
Every treatment has a flip side. Overalkalinizing can cause metabolic alkalosis, while high sodium loads may raise blood pressure. Thats why shared decisionmaking matters.
Benefits snapshot
- Improved growth in children (type1 &2).
- Fewer kidney stones.
- Stabilized potassium, better heart health (type4).
Potential downsides
- Alkalosis if bicarbonate is too high.
- Fluid overload from sodiumheavy meds.
- Medication sideeffects (GI upset, hypertension).
Shared decision checklist
Before you (or your doctor) pick a plan, ask:
- What are the shortterm goals?
- How will we monitor safety?
- What lifestyle changes will make the meds work better?
- Are there other health issues (e.g., diabetes) that could affect treatment?
RealWorld Stories
Let me share a quick story that stuck with me. I once chatted with Maya, a 34yearold accountant who was diagnosed with type4 RTA after routine labs showed a mildly low pH and high potassium. Shed been feeling off for months, attributing fatigue to her busy schedule. Once she started lowdose fludrocortisone and tightened her bloodsugar control, her energy bounced back, and her potassium normalized. Mayas experience taught me that early detection plus a tailored plan makes a world of difference.
Another case: little Tommy, age 7, kept getting bone pain and limpwalking at school. A pediatric nephrologist spotted proximal RTA (type2) and started highdose bicarbonate plus vitamin D. Within a year, his growth chart leaped forward, and the limp disappeared. Stories like these remind us that RTA isnt just a lab number its about real lives.
Trusted Sources
When you dive deeper, these resources keep the info solid:
- clear explanations of each RTA type.
- Recent review in Kidney International (2024) on the genetics behind distal RTA perfect if youre curious about the science.
Always look for uptodate guidelines from reputable medical societies. Theyre the backbone of the EEAT (Experience, Expertise, Authoritativeness, Trustworthiness) principles that help Googleand youspot reliable content.
WrapUp
Understanding the renal tubular acidosis types is like learning the dialects of a language; each has its own accent, but they all belong to the same family. Whether youre facing the stoneforming worries of type1, the boneweakening challenges of type2, or the potassiumladen nuances of type4, the path forward is clear: identify the pattern, tailor the treatment, and stay engaged with your healthcare team.
If anything in this guide sparked a question, or if youve walked a similar path and want to share, feel free to reach out. Knowledge is power, and together we can keep our kidneysand our livesbalanced.
FAQs
What are the main types of renal tubular acidosis?
The main types of renal tubular acidosis (RTA) are Type 1 (distal RTA), Type 2 (proximal RTA), and Type 4 (hyperkalemic RTA). Type 1 involves impaired hydrogen ion secretion in the distal tubule, Type 2 involves poor bicarbonate reabsorption in the proximal tubule, and Type 4 is characterized by aldosterone resistance in the collecting duct with hyperkalemia.
What symptoms suggest distal (Type 1) RTA?
Symptoms of distal RTA include kidney stones, muscle weakness, and in children, growth delays. Lab results often show low urine pH (<5.5) and normal anion gap metabolic acidosis.
How is proximal (Type 2) RTA diagnosed and what are its signs?
Proximal RTA is diagnosed by detecting high urinary bicarbonate loss with variable urine pH, often accompanied by bone pain, rickets or osteomalacia, and increased urination (polyuria).
What causes Type 4 renal tubular acidosis and its symptoms?
Type 4 RTA is usually caused by aldosterone deficiency or resistance, leading to impaired potassium excretion. It presents with hyperkalemia, mild acidosis, fatigue, hypertension, and may be linked to diabetes.
What treatments are common for the different RTA types?
Treatment usually involves alkali therapy such as sodium bicarbonate or potassium citrate to correct acidosis. Type 4 may additionally require fludrocortisone and potassium-lowering strategies. Managing underlying conditions is also essential.