Hey there, friend. If youve just heard the words renal failure medication and feel a knot in your stomach, youre not alone. Lets cut through the jargon and get straight to the heart of what matters: which medicines can actually help your kidneys, which ones you should watch out for, and how to stay on top of your health without feeling overwhelmed.
In the next few minutes well walk through the basics, dive into the major drug families, flag the culprits that can hurt your kidneys, and peek at the newest treatments on the horizon. Think of this as a friendly chat over coffeeclear, honest, and packed with the info you really need.
Understanding Renal Drugs
First things first: renal failure medication isnt a single pill. Its a toolbox of drugs that work together to protect whats left of kidney function, manage the sideeffects of chronic kidney disease (CKD), and keep other organs happy.
These medications fall into a few broad categories:
- Bloodpressure controllers (ACE inhibitors, ARBs, betablockers)
- Glucoselowering and cardiorenal agents (SGLT2 inhibitors, GLP1 agonists)
- Mineralbalance helpers (phosphate binders, sodium bicarbonate)
- Antiinflammatory & immune modulators (steroids, mycophenolate)
- Lipidlowering and heartprotecting drugs (statins, lowdose aspirin)
Each class has its own goals, benefits, and potential pitfalls. Lets break them down one by one.
Why Medication Matters
Imagine your kidneys as a pair of tiny waterfilters. Over time, they get clogged, leaky, or just worn out. Medicines can:
- Slow the decline of filtration (measured by eGFR).
- Control blood pressurethe single biggest driver of kidney damage.
- Reduce protein in the urine, a sign that the kidneys are protecting themselves.
- Manage complications like anemia, bone disease, and high potassium.
But its a balancing act. The same drugs that protect can also tip the scale toward sideeffects if were not careful. Thats why a solid understandingbacked by doctors, guidelines, and a sprinkle of personal experiencemakes all the difference.
What does renal failure medication actually cover?
In short, it includes any prescription or overthecounter (OTC) product that influences kidney function, blood pressure, electrolyte balance, or the progression of CKD. Some drugs are specifically approved for CKD (like certain SGLT2 inhibitors), while others are borrowed from other fields because they happen to help kidneys as a side effect.
Quick reference table
| Drug class | Primary use | Typical stage | Major benefit | Common sideeffects |
|---|---|---|---|---|
| ACE inhibitors / ARBs | Bloodpressure & proteinuria control | 14 | Slows GFR loss | Cough, hyperkalaemia |
| SGLT2 inhibitors | Glucose & cardiorenal protection | 24 | ESRD risk, CV death | UTIs, genital yeast infections |
| Finerenone | Mineralocorticoidreceptor antagonist | 34 | albuminuria, CV events | Hyperkalaemia |
| Phosphate binders | Control phosphorus in stage5 | 5 | Prevents bone disease | GI upset, constipation |
Core Medication Categories
BloodPressure Controllers
High blood pressure is the villain that sneaks up on kidneys. ACE inhibitors (like lisinopril) and ARBs (such as losartan) are the first line of defense. They relax the blood vessels that feed the kidneys, lower protein leaking into the urine, and have been shown in to reduce the risk of reaching endstage renal disease (ESRD).
Typical dosing starts low (e.g., lisinopril 5mg daily) and is gradually titrated. Checking serum creatinine and potassium within a week of starting is essential. If you notice a sudden spike, your doctor may adjust the dose or switch drugs.
Reallife dosing cheatsheet
- Lisinopril: 5mg 10mg 20mg daily.
- Losartan: 25mg 50mg 100mg daily.
- Monitor: Creatinine +30%? Hold dose. Potassium >5.5mmol/L? Reduce or stop.
Diabetes & CardioRenal Agents
If you have diabetes, the spotlight shines on SGLT2 inhibitors (dapagliflozin, empagliflozin). A 2023 FDA approval extended their use to CKD even without diabetestalk about a game changer! These drugs lower blood sugar by making the kidneys dump excess glucose in the urine, but they also reduce inflammation and improve kidney oxygenation.
Whats the latest? A study published in the New England Journal of Medicine showed a 30% reduction in kidneyfailure events for patients on dapagliflozin. Sideeffects are usually mild, like a bit more bathroom trips or a higher chance of yeast infections.
Patient vignette
John, a 58yearold with stage3 CKD and type2 diabetes, added Farxiga (dapagliflozin) to his regimen. Six months later, his eGFR went from 45 to 51mL/min/1.73m and his albumintocreatinine ratio dropped by 40%. I felt like my kidneys finally got a break, he told me, smiling.
MineralBalance & AcidBase Drugs
When kidneys cant clear acids effectively, metabolic acidosis creeps in. Sodium bicarbonate tablets are a simple, inexpensive way to buffer the blood and protect muscle tissue. Phosphate binders (sevelamer, calcium acetate) become crucial in stage5, preventing calciumphosphate crystals that damage bones and vessels.
Whentoprescribe flowchart
- eGFR<30Check serum bicarbonate.
- Bicarbonate<22mmol/L Start oral sodium bicarbonate 650mg TID.
- Serum phosphorus>5.5mg/dL Add phosphate binder with meals.
AntiInflammatory & Immune Modulators
Some kidney diseases, like glomerulonephritis, are driven by the immune system. Steroids (prednisone) can calm the fire, but longterm use brings osteoporosis, weight gain, and mood swings. Thats where steroidsparing agents like mycophenolate or cyclophosphamide step in. The key is a tailored plan that minimizes exposure while keeping inflammation in check.
Comparison: Steroidsparing vs. steroids
| Aspect | Steroids | Steroidsparing agents |
|---|---|---|
| Onset of action | Fast (days) | Weeks |
| Sideeffects | Weight gain, high blood sugar, bone loss | GI upset, infection risk |
| Longterm safety | Limited | Better for chronic use |
LipidLowering & Cardiovascular Protectors
Kidney disease and heart disease are practically twins. Statins lower LDL cholesterol, reducing the extra strain on alreadyfragile vessels. Even in stage4 CKD, moderateintensity statins are recommended unless youre on dialysis, where the benefit tapers off.
Statin dosing adjustments
For eGFR<30, start with a lowtomoderate dose (e.g., rosuvastatin 5mg) and monitor liver enzymes. If youre on a highintensity statin, consider a dose reduction to avoid muscle toxicity.
Medications That Can Harm
Top 10 Drugs That Cause Kidney Damage
Not all pills are friends. Some are outright troublemakers for kidneys:
- Nonsteroidal antiinflammatory drugs (NSAIDs) ibuprofen, naproxen.
- Certain antibiotics aminoglycosides (gentamicin), vancomycin.
- Contrast dyes used in imaging.
- Protonpump inhibitors (longterm high dose).
- Diuretics (highdose furosemide) without monitoring.
- Herbal supplements aristolochic acid, highdose vitamin C.
- Antiretrovirals (tenofovir) in certain populations.
- Chemotherapy agents cisplatin.
- Lithium (used for bipolar disorder).
- Some antihypertensives ACE inhibitors when used in acute kidney injury.
Do I need to stop ___?
Before you yank a pill off the shelf, talk to your doctor. Often the answer is use it cautiously, not quit outright. For example, occasional ibuprofen for a headache isnt the end of the worldbut daily use can be a silent assassin.
Herbal & OTC Pitfalls
People love natural remedies, yet many contain compounds that stress the kidneys. Highdose creatine, raw garlic extracts, and certain traditional Chinese herbs have been linked to acute kidney injury. If youre thinking about a supplement, ask your nephrologist first.
Safe alternatives
- Instead of highdose vitamin C, get antioxidants from berries.
- Swap ibuprofen for acetaminophen (within safe limits).
- Use turmeric as a spice rather than a concentrated capsule.
Emerging New Therapies
Finerenone the New Kid on the Block
Finerenone is a selective mineralocorticoidreceptor antagonist that showed a 20% reduction in kidneyfailure events in the recent FIGARODKD trial. Its especially useful for patients who cant tolerate high potassium levels from ACEI/ARBs.
Talking to your nephrologist
Ask whether finerenone fits your stage of CKD, current potassium levels, and heartfailure status. If youre already on an ACEI, your doctor may start finerenone at 10mg daily and watch potassium closely for the first month.
Upcoming Pipeline: Dual GLP1/SGLT2 Agents
Pharma giants are developing combo pills that hit both GLP1 (for weight loss and glucose control) and SGLT2 pathways (for kidney protection). Early PhaseIII data suggest stronger eGFR preservation than either class alone.
What to expect
These combos may cost more, but insurance plans are beginning to cover them for CKD patients. Sideeffects appear similarmostly mild GI upset and the usual SGLT2related infections. Keep an eye out; approval could arrive as early as 2025.
Practical Medication Guide
Steps to a Safe Regimen
- Make a master listinclude every prescription, OTC, and supplement.
- Check kidney labs before any new drug: eGFR, creatinine, potassium.
- Set a monitoring calendarmost labs every 36months, or sooner after changes.
- Ask the right questions at each visit: Why this drug?, What symptoms should I watch for?
- Stay hydrated, but not overhydratedfollow your doctors fluid recommendations.
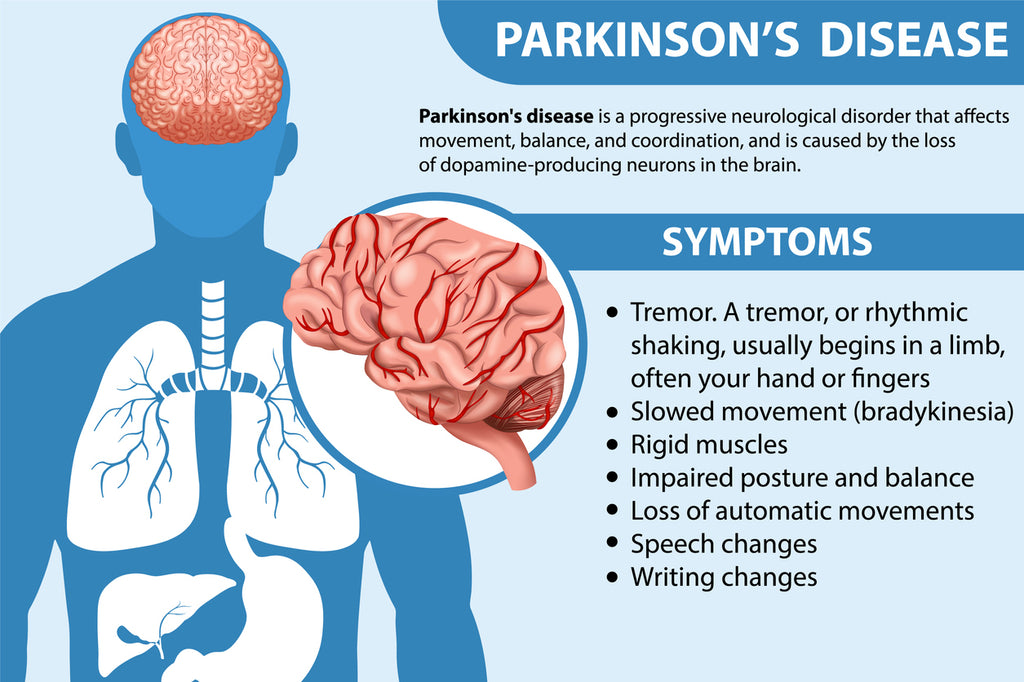
For patients dealing with complications such as overactive bladder, related especially in conditions like Parkinson's disease, understanding symptoms and managing medication effectively is crucial. Exploring resources on manage OAB Parkinson can provide valuable insights into tailored treatment approaches.
Printable medication checklist (editable PDF)
Feel free to download a simple spreadsheet where you can tick off each drug, note the dose, and record the last lab result. Having it on the fridge turns a medical chore into a quick daily glance.
Kidney Failure Treatment Without Dialysis
Dialysis isnt the only path, especially in the early stages. Combining strict bloodpressure control, SGLT2 inhibitors, a lowprotein diet, and regular exercise can often keep you out of the dialysis chair for years.
One friend, Mike, was told hed need dialysis within two years. After a comprehensive medication makeoveradding an ACEI, a lowdose SGLT2 inhibitor, and a phosphate binderhis eGFR plateaued at 28mL/min for three years. He credits the teamapproach and his willingness to adjust lifestyle.
Conclusion
Renal failure medication isnt a mystery locked away in a pharmacyit\'s a set of tools you can understand, question, and use wisely. By knowing which drugs protect your kidneys, which can unintentionally harm them, and staying uptodate with breakthroughs like finerenone, you empower yourself to steer the course of your kidney health.
Take the next step: jot down every medication youre on, schedule that lab check, and bring these questions to your next doctors visit. If youve tried any of these meds or have a story to share, drop a comment below. Were in this together, and every shared experience helps us all stay a little healthier.
FAQs
What types of drugs are classified as renal failure medication?
Renal failure medication includes any prescription or OTC drug that affects kidney function, blood pressure, electrolyte balance, or slows CKD progression—such as ACE inhibitors, ARBs, SGLT2 inhibitors, phosphate binders, and newer agents like finerenone.
How do ACE inhibitors protect the kidneys?
ACE inhibitors relax the blood vessels supplying the kidneys, lower blood pressure, reduce protein leakage into urine, and have been shown to slow the decline of eGFR, delaying the need for dialysis.
Can I use SGLT2 inhibitors if I don’t have diabetes?
Yes. In 2023 the FDA approved SGLT2 inhibitors for CKD patients regardless of diabetes status because they improve kidney oxygenation and reduce the risk of kidney‑failure events.
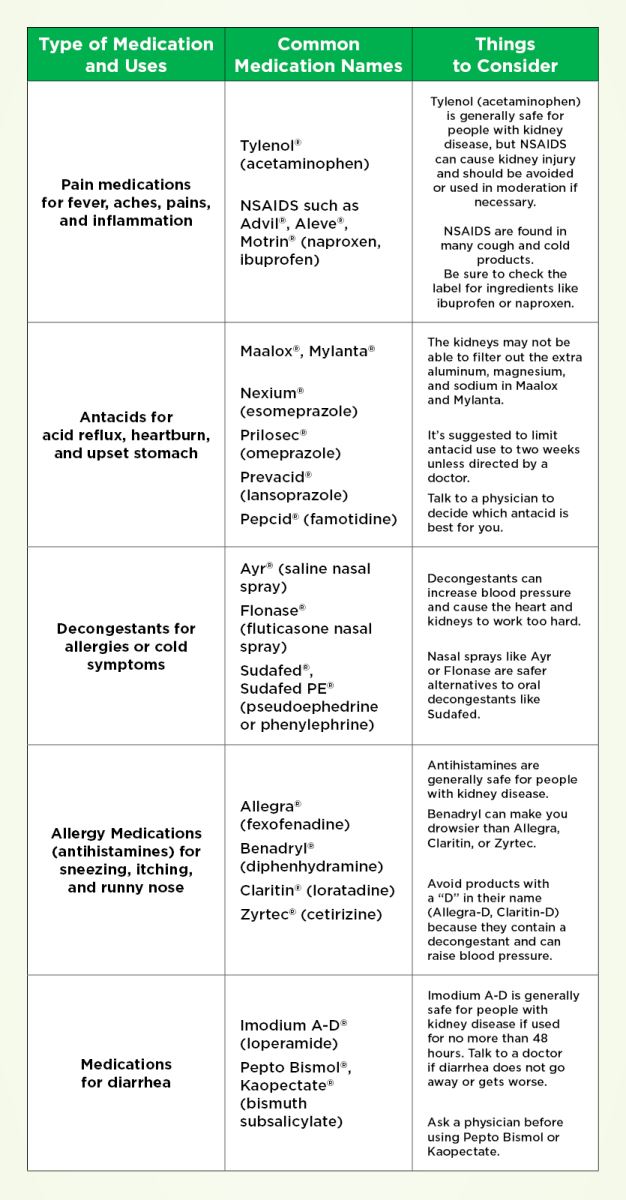
Which common over‑the‑counter drugs should I avoid with kidney disease?
NSAIDs (ibuprofen, naproxen), high‑dose proton‑pump inhibitors, certain antibiotics like gentamicin, and some herbal supplements (e.g., aristolochic acid) can worsen kidney function and should be used only under medical guidance.
What new kidney‑protective drugs are emerging?
Finerenone, a selective mineralocorticoid‑receptor antagonist, has shown a 20% reduction in kidney‑failure events. Dual GLP‑1/SGLT2 combination pills are also in late‑stage trials, promising stronger eGFR preservation.